Size of the Breasts
Copyright 2008
Introduction
The
The size of the breasts varies significantly between individuals and is different in each individual depending on their age and functional state. The normal mature female breast ranges from less than 30 grams to more than 500 grams.
| Average Size |
|
This patient has average sized breasts, contributed mainly by dense stromal and glandular tissue but little adipose tissue. There is a paucity of fat in the rest of her body as well. 25582b01 Courtesy Ashley Davidoff MD |
| Large Breasts |
In this 20 year old female the large size of her breasts is due to very prominent glandular and stromal tissue. Note she has little fat in her breasts and has a paucity of fat in the rest of her body. 42662 Davidoff MD |
Because the breast is a major repository for fat, the size and density of the breast is greatly influenced by diet and muscle development. Difference in size between individuals and differences during different phases of life can be dramatic, and is related to a combination of weight, hormonal influence and genetic factors.
In the young the differences are usually related to hormonal differences and genetics while in the post menopausal women the relationship of breast size to weight and fat distribution becomes more relevant. The hormones mostly responsible for breast changes are estrogen and progesterone.
Estrogens cause fat deposition, duct elongation and branching, development of the stromal tissues, including the connective tissue and blood vessels. They have some effect on the lobules and alveoli but it is progesterone and prolactin that transform the breasts into lactating organs. Progesterone causes the alveoli and lobules to proliferate and enlarge and enable the organ to become secretory, but it is left up to prolactin to provide the final capability of milk production.
Puberty is the first phase of breast maturation. Before puberty the breasts are small, and start to enlarge with the onset of thelarche at about 11 years, becoming fully developed at the age of 15 or 16 years. Early development of breasts has no bearing on the final breast size.
During puberty the anterior pituitary gland produces follicular stimulating hormone (FSH) which causes the follicles of the ovary to produce estrogen. Estrogen causes ductal development and proliferation of periductal fibrous tissues. Both these changes result in the enlargement of the breasts and the increasing firmness.
The second phase of breast maturation occurs with the onset of ovulation when progesterone becomes a factor in breast size. It is produced by the corpus luteum in the second half of the menstrual cycle, and is responsible for the proliferation of the glandular component of the breast development. Under the influence of progesterone stromal fluid accumulation occurs in the last few days of the cycle.
The intrinsic MRI signal differences between parenchyma (glandular tissue and stroma) water and fat makes evaluation of breast changes relatively easy to study using MRI. During a single cycle the parenchyma increases by more than 30%, while water content increases by about 25%. (Fowler)
Hussain found the mean volume of the breasts of 15 healthy females aged between 22 and 44 years was about 560ccs. The author was able to measure the difference in breast size at ovulation where size was relatively small, in the premenstrual phase where size was largest, and in post menstrual phase where regression was measured. Milligan suggested that the overall change in the total volume of the breast over a cycle was about 100mls. (related articles)
Preponderance of Fat |
|
In this 35year old patient the breast has a preponderance of fat with some glandular tissue but very little stromal tissue. She is an average sized patient with an average amount of fat and average sized breasts. Courtesy Ashley Davidoff MD 2548. |
During pregnancy the breasts increase significantly in size, increasing by about 400grams per breast, under the influence of estrogen progesterone growth hormone insulin and cortisol. Prolactin also plays a role of breast enlargement during pregnancy resulting in an overall average increase in size of about 145mls. The higher levels of estrogen result in progressive proliferation, elongation, and dilatation of the ductal system while progesterone is mostly responsible for glandular development. Most of the fat of the breast is replaced in late pregnancy by enlarging glandular tissue necessary to produce milk. The nipple and areola become deeply pigmented and increase in size as well.
 |
| Post Partum Breast |
|
In this recently post partum patient there are no specific features that suggest she is lactating. In her there is a balance of fat, glandular tissue and stromal tissue. Courtesy Ashley Davidoff MD. 42689 |
Following birth and delivery of the placenta there is a sudden drop of estrogen and progesterone levels. Prolactin plays an increasing role in breast function and morphology as milk production is initiated and continued throughout the nursing period.
Non Lactating and Lactating Breast |
|
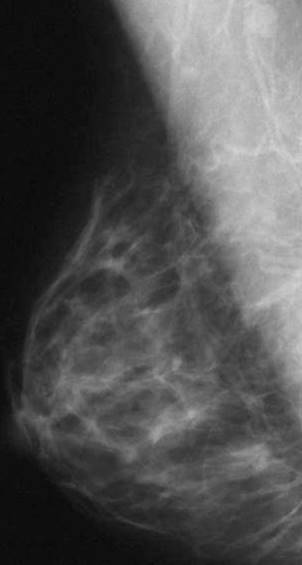
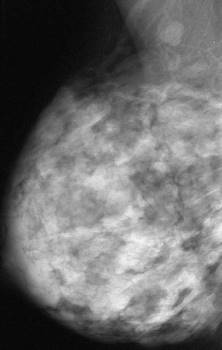
The first image is from a screening mammogramand the second image of the same patient was taken during lactation. Note the change in size and contours of the breast and how the predominant linear pattern of the non lactating breast becomes nodular and lobular with lactation. Courtesy Priscilla Slanetz MD MPH 43064b01 43065b01 |
As the infant starts to suck on the nipple a reflex production of prolactin from the anterior pituitary gland occurs. The prolactin in turn stimulates a cascade of hormonal events with a subsequent cascade of flowing milk. As stated the ducts of the apocrine glands act as storage sites for the milk produced by the acini. The breasts, are larger by about 10-20% as they become distended with milk (Dewey) In the first two days post partum there is only about 50ccs per day of milk produced, which increases dramatically to 500ccs per day by day 4. At 3 months post partum this usually plateaus at 850-1000ccs per day. If the mother feeds every 4 hours then at peak production prior to feeding there should be about 120ccs of milk in the breasts equating to about 50-60ccs per breast. (related links) The rate of milk production has been estimated at between 10-60ccs per hour (Daly) The basic size of the breast has no bearing on the volume of milk. At the peak of lactation the breasts become almost double their baseline size.
With advancing age glandular and stromal tissue atrophies but fatty tissue may become quite abundant. The breasts may become very large in post menopausal life due to fat accumulation. Hormonal supplementation may cause added increase in size. In advanced age the breasts usually shrink as the fat regresses.
Psychologically the size of the breasts to some cultures and individuals has been linked to sexuality. Breast augmentation both enlargement and reduction, is a well known and accepted method used for psychological benefits. (related articles)
 |
| Implants |
|
This middle aged lady chose to enlarge her breasts for cosmetic reasons. The implants are filled with saline. Courtesy Ashley Davidoff MD 42702 |
In summary, the size of the breasts relates to a combination of the quantity of fat, glandular tissue and stromal tissue. The glandular, ductal, and stromal tissues change by month, with growth and regression while under the influence of estrogen and progesterone. The amount of fatty tissue relates to a combination of hormonal, hereditary, racial factors, nutritional factors, body size, and age. Overweight patients for example tend to have larger breasts. Applied Anatomy
The breasts in up to 50% of women are unequal in size. (Loksen). Difference in size may occur during development and may become symmetrical with maturation. The left breast is generally a little larger than the right. (Loughry)
Asymmetry |
|
In this elderly lady there is obvious asymmetry between the two with a larger right breast. It is more common to have the left breast be the dominant breast. Courtesy Ashley Davidoff MD 42685 |

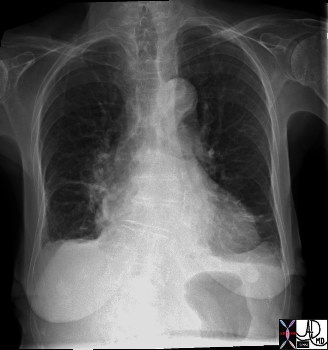
Asymmetric Size |
| 71175c01 aorta thorax thoracic fx aortic ectasia sigmoid shape tortuosity breast asymmetry size CXR plain film Davidoff MD |
| Surgical Absence |
|
In this patient the left breast is surgically absent due to removal for cancer. Courtesy Ashley Davidoff MD 41783b |
The glandular tissue is not uniformly distributed within the breast. The axillary parenchymal tissue is thickest followed by the inferior aspect, sternal aspect and then the clavicular aspect. This dominance of tissue in the upper outer quadrant has clinical relevance. Cyclical discomfort is most commonly felt in this region, and about 50% of carcinomas occur in this region as well.
Variation in Fat and Glandular Components |
|
In this 31 year old female patient the non uniform distribution of the parenchyma is well demonstrated. Note the large amount of parenchyma (glandular and stromal tissue) in the axilla and the very obvious thinning medially. This is the normal distribution of the parenchyma. Courtesy Ashley Davidoff MD 42675 |
Congenital absence of the breast does occur but is rare (Martinez-Chequer). It is called amastia. When it is unilateral it often occurs with ipsilateral absence of the pectoralis muscle. When it is bilateral it is usually associated with other anomalies. Reference to amastia is thought to be present in the Songs of Solomon “We have a little sister, and she hath no breasts” (Song of Songs VIII:8).
Polymastia on the other hand occurs in between .2 – 2% of females, and less commonly among males. It is characterized by accessory breast tissue that occurs along the milk line starting in the axilla, proceeding with an anterior arc through the normal nipples, and ending in the groin. Hormonal changes and diseases that affect the normal breast can affect the accessory breast tissue as well. If there are accessory nipples without breast tissue the condition is called polythelia or supernumary nipples. (Sadove)
The number of breasts differs among mammals. Humans and guinea pigs have two, cows have 4, cats have 8, and dogs 10. The size of the breasts also differs significantly among mammals and bears no relation to the relative size of the animal. Cows have enormous udders while horses have relatively small breasts. Goats also have breasts that are relatively large compared to sheep that have relatively small breasts.
The testes normally secrete circulating estrogen produced in small amounts but it is rapidly and effectively metabolized by the liver so that in health there are no overt estrogen effects on the male body. However in liver disease, when the liver is unable to catabolize the estrogen, excess estrogen circulates which may cause breast growth. This condition is called gynecomastia. There are other stages in the normal male such as in puberty and old age where excess estrogen causes breast tissue proliferation. In the pubescent male this may be unilateral or bilateral but is usually self limiting after a few months but may be present for up to three years. In obesity there is also an excess of estrogen which may have the same effects on the male breast. Certain drugs such as anabolic steroids illegally used by athletes as well as other illegal drugs such as marijuana and heroine can also cause gynecomastia. Drugs used in the cardiovascular system including digoxin, spirinolactone and reserpine are well known causes of gynecomastia.
 |
| Gynecomastia |
|
This mammogram of a male breast shows gynecomastia with enlargement of both adipose components and subareolar fibroglandular tissue. Courtesy Priscilla Slanetz MD MPH 42795 |
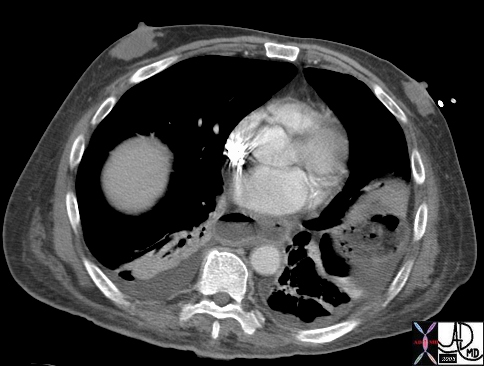 |
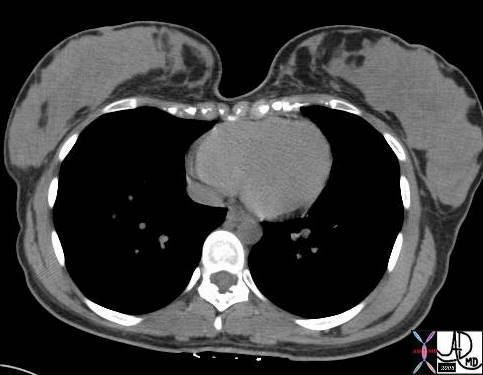
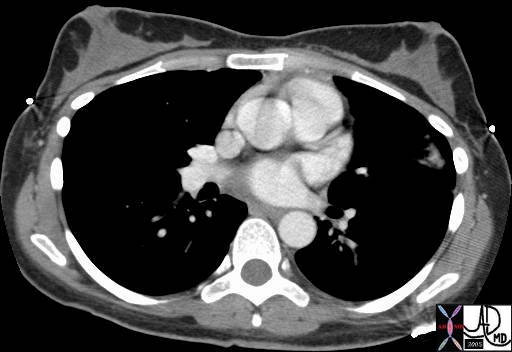
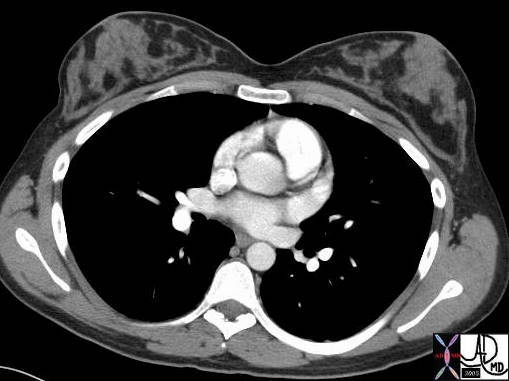
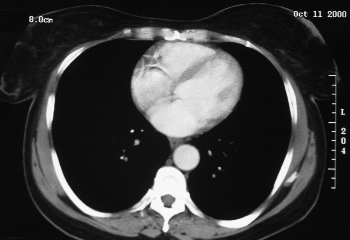
| Gynecomastia |
| This is a cross sectional CTscan of the chest of a very ill 70 year old male with bilateral gynecomastia characterized mostly by fibroglandular proliferation. Associated findings of bilateral pleuroparenchymal changes in the lungs and a dilated esophagus are of note. Courtesy Ashley Davidoff MD 43663 |
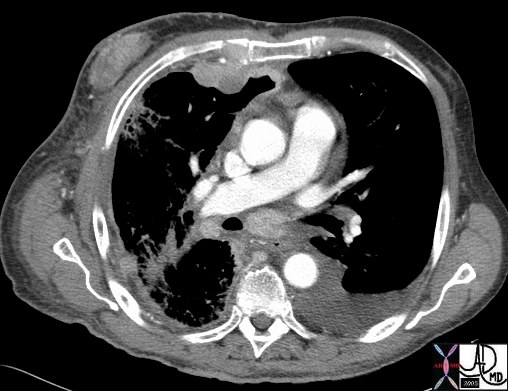
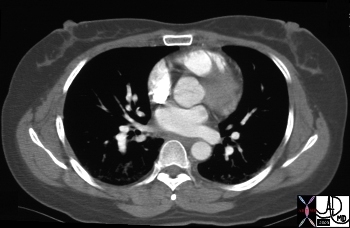
Radiation Mastitis |
| In this 76 year old male there is unilateral enlargement of the breast with overlying skin thickening and induration. The patient has right sided lung cancer and was treated with radiation. The enlargement of the breast is thought to be secondary to radiation mastitis. Courtesy Ashley Davidoff MD 43659 |
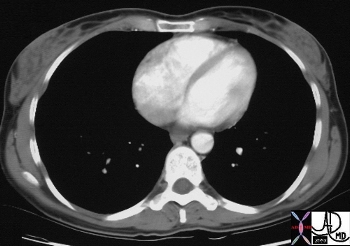
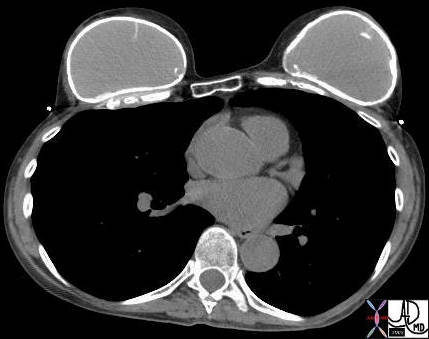
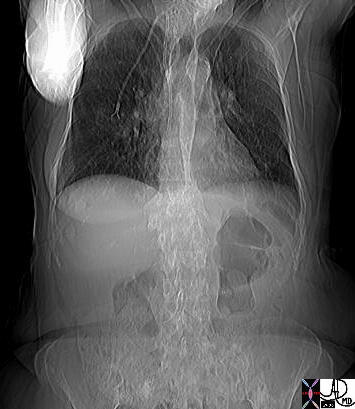
Hormonally Induced Breast GRowth – Gender Identity Disorder |
| This is a CT scan of a male patient with a gender identity disorder who desired large breasts. The use of hormonal supplementation resulted in proliferation of the adipose tissue. The large breasts are not easy to see since they have no soft tissue.
Courtesy Ashley Davidoff MD 20385 |
The overlying skin of the breast should be less than 3mm thick. This has important implications in the evaluation of the breast in mammography since thickening of the skin implies a pathological process.
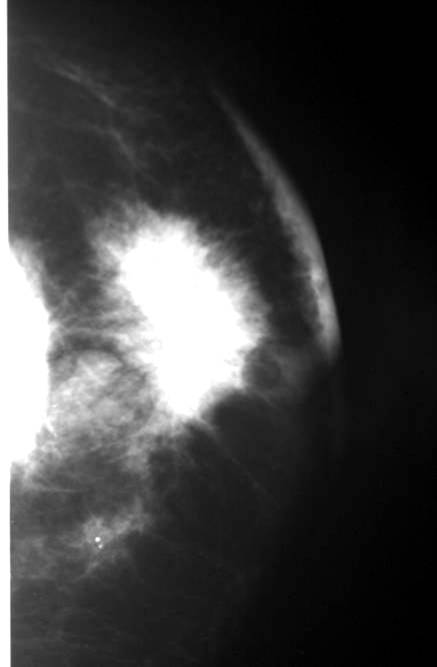 |
| Skin Thickening |
| This patient has rapidly advancing inflammatory breast carcinoma with a mass seen in the right breast with overlying skin thickening and underlying pectoralis muscle involvement. Courtesy Priscilla Slanetz MD MPH. 42987 |