The Common Vein Copyright 2008
Author Lisa Wiechmann MD
Overview
The current favored hypothesis on the evolution of breast cancer describes a progression similar to that in colon cancer ( Knudson’s hypothesis) that includes usual ductal hyperplasia, atypical hyperplasia, carcinoma in situ ( ductal carcinoma in situ and lobular carcinoma in situ) and invasive carcinoma. The term of carcinoma in situ of the breast is used to describe cancer cells that don’t invade the basement membrane. Each type of breast carcinoma in situ (DCIS and LCIS) has a distinct clinical and biological behavior. DCIS is defined as the proliferation of epithelial cells confined to the mammary ducts without demonstrable invasion through the basement membrane.
Ductal carcinoma in situ (DCIS), also known as intraductal carcinoma, is found in approximately 7% of all biopsied specimens It is considered a premalignant condition and risk of invasive breast cancer
is increased nearly five times in women with DCIS. Such risk is primarily ipsilateral as a pose to LCIS which is more likely to be multifocal and bilateral. Multicentricity is seen in 60-90
% of patients with LCIS and in 40-80% of patients with DCIS. LCIS occurs bilaterally in 10-20% of of DCIS cases and in 50-70% of LCIS cases.
Before mammography DCIS was primarily diagnosed by physical examination as a palpable lesion. In situ breast cancers constituted approximately 2% of all breast cancers in 1980 and LCIS was more common than DCIS by a ratio of 2:1. Screeing mammography revealed a 14 fold increase in the incidence of in situ cancer (45%) and DCIS was diagnosed more frequently than LCIS.
Classification
Many different vriants of DCIS have been described. The traditional classification system is based on the architectural pattern of the lesion and identifies five major subtypes: comed , cribriform, micropapillary, papillary and solid. Comedo type DCIS is characterized by the presence of necrosis, cribriform DCID has a fenestrated proliferation fo neoplastic cells, the micropapillary type features groups of cells orieted perpedicular to the basement membrane; the papillary type of DCIS demonstrates intraluminal projections that have central fibrovascular cores( true papillae) and finally the solid type of DCIS the tumor cells fill the involved area without any of the above described architectural patterns.Apocrine DCIS, intraductal signet cell carcinoma , endocrine DCIS and solitary papillary carcinoma are rare variants that are at times identified.
More recently Lagios et al proposed a classification based on nuclear grade and necrosis as a pose to architectural characteristics. Three major categories of DCIS are based on a modification of this system : high , intermediate and low grade DCIS. In 1997 a consensus conference was assembled in attempt to identify a classification system that was clinically relevanta and reproducible: although the panel did not endorse a specific system, it was agreed that certain features be routinely documented in pathology reports of DCIS: these included the presence of necrosis ( comedo or punctuate) , nuclear grade (low, intermediate of high) , cell polarization and architectural pattern.
Statistics
DCIS represents approximaately 70% of noninvasive carcinomas and its incidence is now 10-20 per 100,000 woman years. Since the introduction of screening mammography the reported incidence( or detection rate) of DCIS has increased significantly and DCIS now accounts for 20-44% of all new screen detected breast neoplasms. Approximately 10-35% of patients with DCIS have a positive family history of breast cancer ( same as for invasive breast cancer). The epidmiology of DCIS reflects that of Invasive breast cancer. SEER ( surveillance, Epidemiology and End Results) data estimated a slightly higher liftime risk of breast cancer for white women ad identified a positive association with higher socioeconomic status.
Geogrpahic Distribution
The incidence of breast cancer varies significantly among differennt countries, and is highest in Northern European countries and in the United States, intermediate in Southern America and Southern and Eastern Europe, and lowest in Asia (Japan, Singapore and urban China have seen a rise in rates with the advent of Western-style economy). Breast cancer incidence and mortality vary sigificatly within the United States. The incidence of breast cancer appears to be highest in white women from Hawaii (128:100,000) followed by those from San Fransisco and the Northeast.The lowes incidence is found in Utah(98:100,000) and New Mexico
The variation of incidence for African-American woment is relatively small ( 94-106:100,000).
Socieconomics
Unlike most other illnesses a positive correlation has been noted between the lifetime risk of breast cancer and higher socioeconomic status.
Genetics
The genetics of DCIS parallel those of invasive breast cancer. Only 5-10% of breast cancers are thought to result from inheritance of a mutated gene. Many Autosomal Dominant conditions have been associated with an increased risk of breast cancer and these include Li-Fraumeni Syndrome, Muir-Torre Syndrome, Cowden disease and Peuts – Jeghers syndreome. Particular attention has been given to BRCA-1 ad BRCA-2 mutations and their association with breast cancer. BRCA-1 is a gene found on the long arm of chromosome 17q wherease BRCA-2 is found on chromosome 13. BRCA- 1 mutations are associated with and increased risk of both breast cancer ( 37-87% by age 70) and ovary (11-42% by age 60) and almost all mutations are found in the germline. BRCA-1 has been associated with orderly and efficient progression of the cell through its life cycle and it appears to play an important role in response to DNA damage. BRCA-2 mutations are associated with a 6% lifetime risk of male breast cancer. The biological function of the BRCA-2 gene is not well understood but it is thought to play a role in DNA damage response. Other types of cancer are associated with mutations in BRCA-2. These include prostate cancer, bladder cancer, pacreatic cancer, Non-Hodgkin’s lymphoma, basal cell carcinoma and fallopian tube tumors.
Sex Distribution
DCIS is almost exclusively a female disease
Age Distribution
The median age of patients with DCIS ranges from 47 to 63 years.
Pathogenesis
The current favoured hypothesis on the evolution of breast cancer describes a progression similar to that in colon cancer ( Knudson’s hypothesis) that includes usual ductal hyperplasio, atypical hyperplasia, carcinoma in situ ( ductal carcinoma in situ and lobular carcinoma in situ) and invasive carcnioma.Malignant cells proliferate and obstruct the ductal lumen thereby may determine an inflammatory reaction, lymphoid infiltration or stromal response around the duct. Certain factors have been identified as indicative of an aggressive biology and such factors include comedo necrosis and high nuclear grade.
Natural History
The most important issue in the management of DCIS is the risk of its progression to breast cancer. Historically DCIS was treated with mastectomy and therefore the question has remained unansweres. Overall the available data quotes a 25-35% risk to develop ivasive breast cancer in the setting of DCIS at 5-10 years.
Gross Pathology
DCIS can be multifocal ( two foci separated by 5mm of normal breast tissue in the same breast quadrant) and multicentric ( a separate focus outside the index quadrant- 30-40%). DCIS of the comedo type is characterized by necrosis which grossly appears as pasty material exuding from the cut surface of the specimen or expressable from the involved ducts by palpation.
Histopathology
DCIS can by divided into subtypes based on architecture and nuclear grade.
The comedo pattern demonstrates prominent necrosis with cells that are large and show nuclear pleomorphism. The necrotic material becomes calcified and can be detected mammographically as linear calcifications. Mitotic figures are numerous and evident including abnormal ones.
Thw cribriform pattern is characterized microscopically by a fenestrated growth of neoplastic cells and radiologically by fine, scattered calcifications.
The micropapillary pattern is characterized by micropapillae without a fibrovascular core that are perpendicular to the basement membrane and project into the ductal lumen. The nuclei are usually monomorphic.
The papillary pattern is characterized by true papille ( with fibrovascular cores) that project into the lumina.
The solid pattern is charcterized by clumps of cells that lack the above specifics.
Apocrine DCIS, intraductal signet cell carcinoma , endocrine DCIS and solitary papillary carcinoma are rare variants that are at times identified.
Cytopathology
Neoplastic cells in DCIS are characterized by varying degrees of cellular atypia: nuclear grade appears to be a predictor of local recurrence.
Clinical Presentation
Before the establishment of screening mammography most patients with DCIS presented with a palpable mass, Paget’s disease of the nipple or nipple discharge. Currently “mammographic” DCIS is more commonly seen.
Imaging
Mammography is the imaging method of choice. Microcalcifications that are evident on mammograms are more commonly seen in comedo type DCIS and are described as linear branching microcalcifications. Presence of a soft tissue mass is unusual.
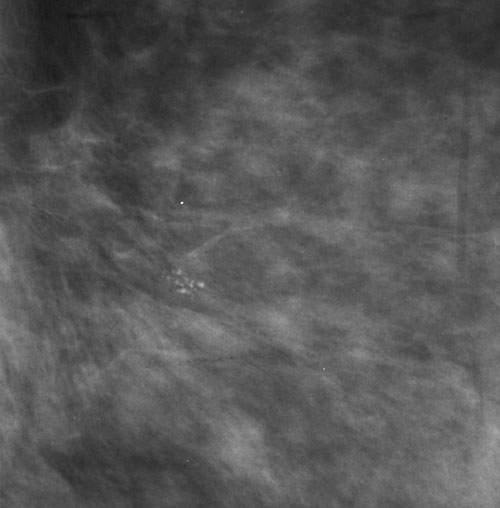
42739 Case 3 DCIS focal RCCmag Courtesy Priscilla Slanetz MD code breast fx calcifications microcalcifications dx DCIS mammogram mammography
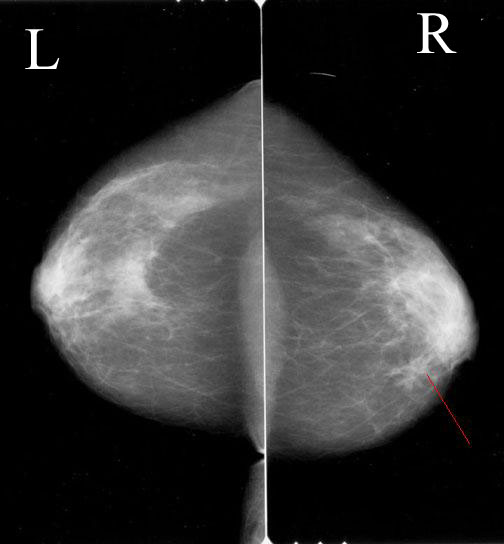
42736 Case 3 IDC with DCIS CC Overlay Courtesy Priscilla Slanetz MD code breast fx mass dx intraductal carcinoma dx DCIS mammogram mammography