Lymphatic Drainage
The breast has a very rich supply of lymphatics, with the dominant flow being toward the axilla. The lymphatics originate in the lobules, and they accompany the veins and ductal systems coursing toward the nipple and areola. An extensive network develops in the subareolar region called the subareolar plexus.
There are about 35 nodes that drain the breast and they are basically divided into 4 regions. The axillary nodes are the largest group and they drain about 75% of the breast. The other major groups include the parasternal group, the infraclavicular group, and the supraclavicular group.
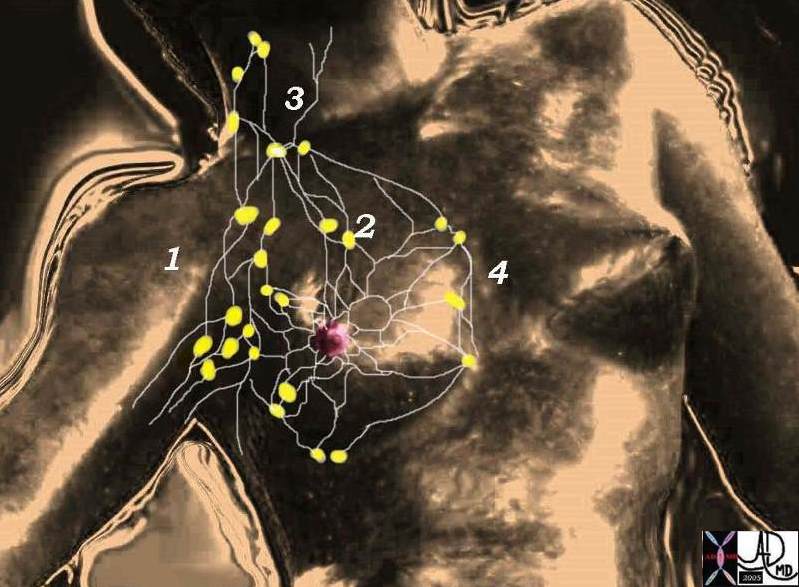 Lymphatic supply of the breast Lymphatic supply of the breast |
| There are 4 basic groups of lymph nodes the largest of which are the axillary group (1) which account for 75% of the lymphatic drainage. The other groups are the infraclavicular (2), supraclavicular (3), and parasternal (4) groups of nodes. Davidoff MD. 78378pb06l05 |
Subgroups of the axillary system of nodes
There are subgroups of the axillary nodes that mostly lie alongside the veins described above. The first of these is called the anterior pectoral group (aka low axillary nodes), consists of about four nodes, and are distributed alongside the lateral thoracic vessels on the lateral border of the pectoralis muscles. The nodes that lie along the axillary vein are called the central axillary nodes. The nodes that lie alongside the subclavian vein are called the subclavian nodes.
There is a set that is not necessarily associated with any specific vein that lies deep to both pectoral muscles under the breast. This group is called the deep fascial system and they drain into set of nodes between the pectoral muscles called Rotter’s nodes. Subsequently some of these nodes will drain into the subclavian nodes and some will drain medially into the internal mammary system which finally drains into the mediastinal nodes.
The other regions described including the infraclavicular, supraclavicular and internal mammary lymphatic drainage are less dominant sites.
Even more uncommon is drainage to the infradiaphragmatic nodes.
It should also be noted that there are intramammary lymph nodes that sometimes masquerade as a breast mass since they have features. On mammography they are typically reniform in shape, have a fatty or radiolucent notch, are less than 1 cm in size and are usually in upper outer quadrant. Cyrlak describes a case of an enlarged intramammary node that turned out to be a site of metastatic involvement of breast carcinoma.
Applied Anatomy
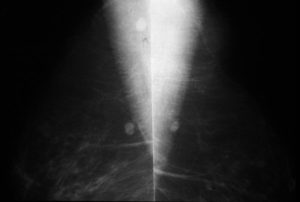
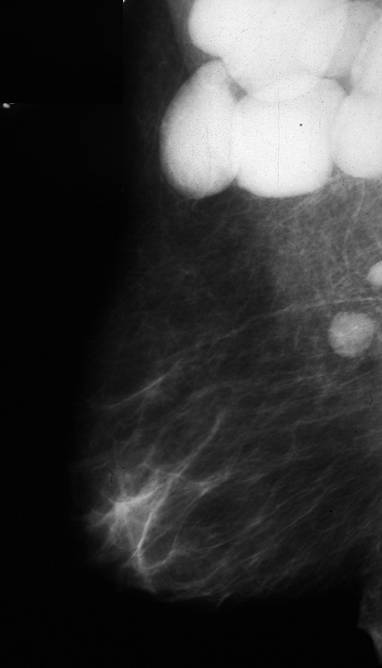
In the following mammogram and intramammary node is seen.
|
|
|
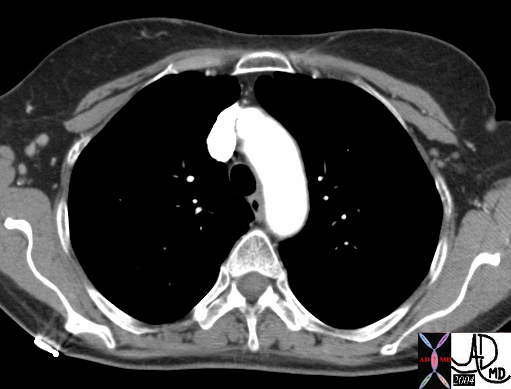
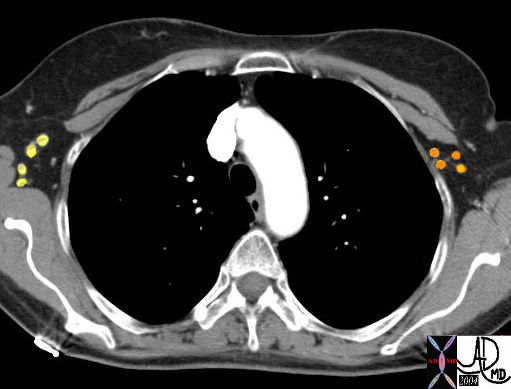
| This is a CT scan of a 62year normal female that shows axillary nodes on the right. These nodes are considered “level 1” lymph nodes in surgical terminology (yellow). They lie lateral to the pectoral muscles. On the left the nodes in orange are level 2 nodes and they lie deep to both pectoral muscles. They belong to the group called the deep fascial system. Courtesy Ashley Davidoff MD 43843 43843b02 |
 Lymph nodes
Lymph nodesThe staging and hence the management of breast carcinoma depends to a large extent on whether the lymph nodes of the breast are involved. Most of the search for disease is directed to the axillary group of nodes. Clinical examination is the first step, mammographic findings the second, sentinel node evaluation using radiopharmaceuticals the third, and surgery and microscopic evaluation the fourth. In cancers involving the medial breast tissue, when the axillary nodes are negative the internal mammary chain is involved in only about 15% of cases, and in lateral cancers the internal mammary nodes are only involved in about 5% of cases.
This mammogram reveals large and dense nodes in left axilla. This patient had leukemic involvement of these nodes. Courtesy Priscilla Slanetz MD MPH 43000b
Lymph nodes
This mammogram reveals large and dense nodes in left axilla. This patient had leukemic involvement of these nodes. Courtesy Priscilla Slanetz MD MPH 43000b
The sentinel node is defined as the first lymph node to drain a region of the breast and in the setting of breast carcinoma would be the first node to contain metastatic disease.
The Sentinel Node Evaluation
Axillary Node Evaluation
Surgical approach to lymph node dissection and resection requires dividing the nodes into 3 levels, going in general from lateral to the breast, to deep and under the breast and pectoral muscles, to deep and medial to the breast. More specifically, a level I dissection is bordered by the axillary vein superiorly, the lateral border of the pectoralis major and minor muscles medially, and the latissimus dorsi muscle laterally. A level II dissection includes nodes below the pectoralis minor muscle, and a level III includes nodes medial to the pectoralis minor muscle and below the costoclavicular ligament. In general if a patient requires lymph node dissection, resecting nodes from Level I and II is considered adequate.
If the nodes are clinically negative then the approach is to evaluate the sentinel node which is the node or group of nodes that drain from the breast to the axilla. Sentinel node identification is evaluated by injecting a small dose of low level radioactive technetium 99 and isosulfan blue dye into the skin in the region of the tumor prior to surgery. A period of between 1-8 hours allows the blue dye and tracer to be taken by the lymphatic system to the regional nodes. A hand held gamma ray counter allows the surgeon to identify the sentinel node. A small incision is made over the radioactivity and between 1 and 3 nodes are removed and given to the pathologist. By this means only limited dissection of the lymph nodes is attained with reasonable certainty that if the sentinel nodes are negative then nodes more distal are negative. If it the sentinel node is positive the tumor is upstaged and further dissection of the lymph nodes required. In the past all axillary nodes would have been removed with consequent morbidity, including significant swelling of the arm from lymphedema and consequent cellulitis.