|
Imaging the Breast
Mammography
Author Priscilla Slanetz MD MPH
A learning module called NOTES SCALES AND MUSIC produced by Charles Allison MD is available to teach the method and art of reading the mammogram
Aim:
Mammography is an x-ray technique designed to detect cancers at an earlier stage than physical examination. Earlier detection translates into earlier stage cancer, and hence, improved long-term prognosis. Most cancers detected by mammography are non-palpable and are ductal carcinoma in situ, which is highly curable.
Indications:
Current screening guidelines are based on a patient’s individual risk. For the average woman, annual mammography starting at age 40 years is recommended. If the patient is high-risk (i.e. has a first degree relative diagnosed with breast cancer), she should begin screening a decade prior to the relative’s age at diagnosis or 40 years, whichever is soonest. Women who are known carriers of the BRAC-1/BRCA-2 mutations often begin screening in their 30’s as they have an 80% lifetime risk of developing breast cancer (10-12% lifetime risk for average patients). Nearly 40% of women treated with mantle radiation for Hodgkin’s disease prior to the age of 25 years will develop breast cancer by age 45, so these women begin annual screening mammography in their 30’s as well.
Diagnostic mammograms are indicated if a patient has a specific problem, such as pain, lump, thickening, or nipple discharge. This examination is performed on symptomatic patients over the age of 30 years and is usually combined with an ultrasound targeted to the area of concern.
Contraindications:
The benefits of any imaging test should always outweigh the risks. In general, there are no true contraindications to mammography. However, mammography is not performed on women who are in the first trimester of pregnancy (unless there is substantial clinical suspicion for breast cancer) or who have an active mastitis. As patients must be able to sit or stand upright, bedridden patients can not undergo the examination.
Advantages:
In multiple randomized screening studies, mammography has been shown to reduce breast cancer mortality by up to 30%. This mortality reduction even applies to women in their 40’s, and more recent studies suggest that these women may benefit even more with reductions up to 45%.
Disadvantages:
For the rare patient, the breast compression associated with mammography is extremely painful and can not be tolerated. If this is the case, the patient is asked to take motrin or ibuprofen an hour prior to her appointment and to schedule the study during the first week of the menstrual cycle (if applicable).
Method
Patient Preparation:
Patients are requested not to wear antiperspirants or powders on the day of the study as the metals in these compounds can appear similar to microcalcifications. Deodorants are usually do not interfere with the images. Patients are also asked to bring all of their prior outside mammograms with them to their appointment as the radiologist will need these as they interpret the current study.
Technique:
The patient is asked to undress from the waist up and put on a gown. The technologist takes the patient into a mammography room and reviews the patient information sheet for accuracy and completeness. Each breast is then positioned for the craniocaudad (CC) and mediolateral oblique (MLO) views. The patient waits until the technologist determines that the images are of good quality. She then can leave the center. The radiologist will interpret the screening study later that day. If the patient has a symptom, she will wait at the center until the radiologist reviews the films, as there may be a need for additional mammographic views or possibly even an ultrasound.
Results:
Recall for additional imaging from a screening examination ranges from 3-12% depending upon the center. The positive predictive value of biopsy for most centers ranges between 20-40%.
The false negative rate of mammography is approximately 5-15%, depending upon the experience of the interpreting radiologist. Double reading (i.e. two radiologists interpret every screening study) and/or the use of computer-aided detection (CAD) can help reduce the false negative rates by up to 40-60%.
Conclusions:
Mammography is a safe, effective tool for the early detection of breast cancer and reduces mortality from breast cancer by up to 30%.
Ultrasound of the Breast
Aim:
Ultrasound uses sound waves to image the breast. This modality is predominantly designed to differentiate a cystic mass from a solid mass. In addition, ulrasound can be used to guide percutaneous procedures, such as fine needle aspiration, core needle biopsy, or percutaneous excision.
Indications:
Ultrasound is indicated to: 1) Evaluate a palpable abnormality on physical exam (focal pain, lump, thickening); 2) Evaluate a mammographic finding (focal mammographic lesion); 3) Evaluate focal pain persistent for greater than 3 months; or 4) To guide a percutaneous procedure such as a core biopsy or fine needle aspiration (FNA). Although there are a few studies using ultrasound to screen for breast cancer, this is not widely embraced as the modality is highly operator dependent. In addition, there are no large randomized studies showing that screening ultrasound reduces mortality from breast cancer.
Contraindications:
There are no known contraindications to breast ultrasound.
Advantages:
Ultrasound is a safe technology with no known side effects. It does not require breast compression. Although usually performed with the patient supine or supine oblique, it can be performed in the upright position in wheelchair bound patients. It offers a means to better characterize palpable and mammographic findings and provides a mechanism to biopsy lesions percutaneously.
Disadvantages:
Ultrasound is highly operator dependent. Despite standard planes to image abnormalities, the detection of an abnormality depends on the skill of the operator. Although there are features on ultrasound which favor benign disease from malignancy, ultrasound can not reliably differentiate solid lesions, and therefore, biopsy is often necessary.
Method
Patient Preparation:
There is no particular preparation for this examination, except that we do ask patients to bring all previous breast imaging studies with them to their appointment.
Technique:
Usually, the patient is asked to lie down on a stretcher. With their arm above their head and in a supine or supine oblique position, the technologist or radiologist places gel on the skin and scans the patient with a linear 12-17MHz transducer in the radial and antiradial planes. Images are usually acquired in both planes if an abnormality is identified and only in one plane if the study is normal. If there is a palpable abnormality, the patient is asked to put their finger on the spot prior to scanning.
Results:
Ultrasound has high specificity for the diagnosis of simple cysts.
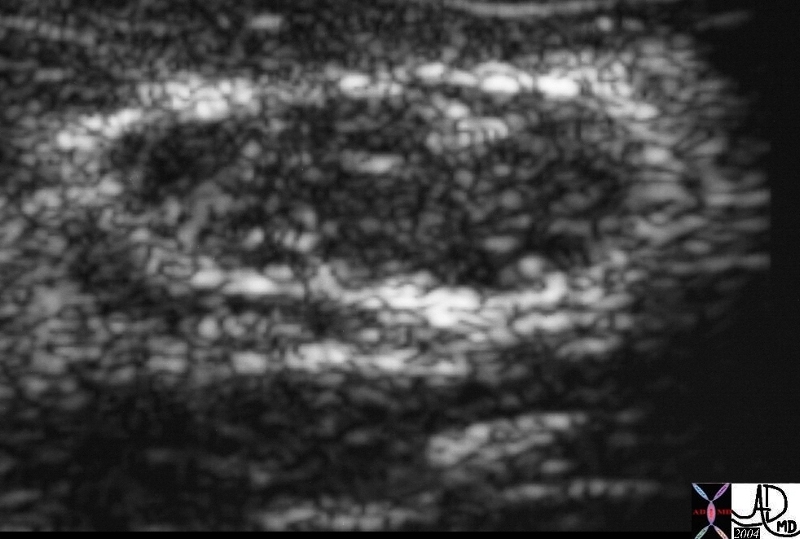
This a an Us of a solid lesion of the breast. In his case the lesion was a fibroadenoma22260 Courtesy Ashley Davidoff MD code breast fx mass fx solid imaging radiology USscan DB
Conclusions:
Ultrasound is a safe modality to evaluate a palpable abnormality or a suspicious mammographic finding. It can reliably differentiate cysts from solid masses.
MRI of the Breast
Aim:
Magnetic resonance imaging (MR) of the breast uses a high-field magnet to image the breast. Multiplanar imaging with different sequences prior to and following contrast administration permits evaluation of the breast tissue. Interpretation of MR studies entails a combination of lesion morphology and enhancement pattern. Lesions that demonstrate early rapid uptake of contrast with a plateau or delayed washout over time are most suspicious for malignancy and warrant biopsy. Gradual uptake of the contrast over time favors a benign process.
Indications:
Current indications for this study are as follows: 1) To determine the integrity of silicone breast implants; 2) To determine disease extent in a newly diagnosed breast cancer patient, particularly younger patients with dense tissue; 3) To identify the breast primary in patients with positive axillary lymph nodes and negative physical exams; 4) To differentiate scar from recurrence in selected patients previously treated for breast cancer; 5) To further characterize an incompletely evaluated suspicious mammographic finding; 6) To monitor response to neoadjuvant chemotherapy in patients with locally advanced breast cancer; and 7) To screen high-risk women, particularly BRCA-1 and BRCA-2 known carriers.
Contraindications:
The standard contraindications to MR imaging apply. In addition, as intravenous gadolinium is given for almost all studies, an allergy to gadolinium would preclude this examination. Relative contraindications include pregnant women as the safety of gadolinium to the fetus is unknown.
Advantages:
MR imaging of the breast is a highly sensitive test with sensitivities approaching 100% for the detection of invasive carcinoma.
Disadvantages:
The specificity is variable depending upon the specific sequences employed and the experience of the interpreting radiologist. In addition, the imaging sequences are not standardized across sites in the U.S..
Method
Patient Preparation:
Patients must be screened for contraindications to MR imaging. Premenopausal patients and cycling postmenopausal patients should be imaged between days 5-15 of the menstrual cycle in order to control for hormonal fluctuations.
Technique:
The patient lies prone on the scanner with her breasts pendent and in mild compression in the dedicated breast coil. An intravenous line is placed through which contrast will be administered. Every center utilizes different sequences for imaging the breasts. In general, most centers acquire images in the sagittal and/or axial plane prior to and following contrast administration. During the contrast injection, dynamic imaging is performed such that images of the entire breast volume are acquired every 1-2 minutes for up to 8-10 minutes following the start of the injection. Using CAD software (Confirma or DynaCad), the enhancement curves can be generated. The entire study usually takes approximately 30 minutes to perform. The radiologist then interprets the images by looking at the lesion morphology and its enhancement pattern.
Results:
MR imaging of the breasts is a highly sensitive test with sensitivities approaching 100% for the detection of invasive carcinoma. Its sensitivity for ductal carcinoma in situ ranges between 10-90% depending upon the center and its sequences. Specificity for this study ranges between 75-90%, once again depending on the specific sequences employed. The false negative rate of MR is unknown.
Conclusions:
MR imaging of the breast serves as a useful adjunct to other breast imaging modalities and for screening high-risk women, particularly known carriers of BRCA-1 and BRCA-2. MR-guided percutaneous core needle biopsy is now available at most centers permitting minmally invasive diagnosis of suspiciously enhancing lesions detected only on MR imaging.
|