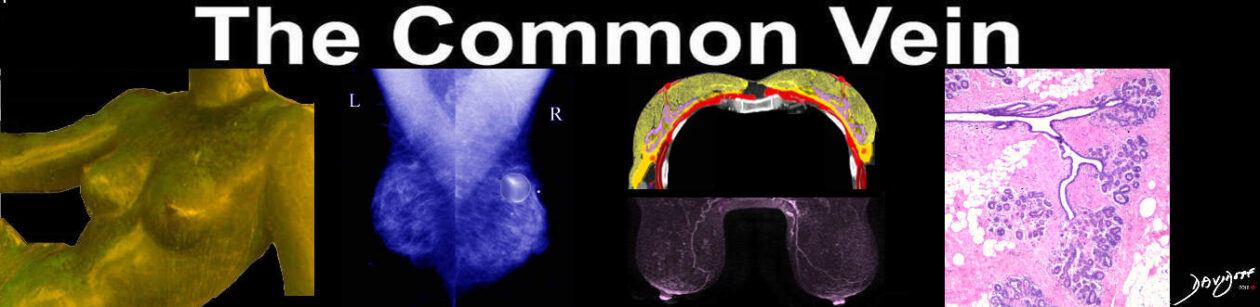
| Shape
Like the size of the breast, the shape of the breast is very varied and depends upon genetic factors, racial factors, dietary factors, age, parity, and menopausal status. However in general the shape of the breast is almost hemispheric, with the superior surface arising more gradually from the chest wall. The superior border is relatively long and flat (sometimes minimally concave) and the inferior border is rounded and shorter. The shape of the breasts changes during each physiologic phase of the female. In infancy there is a variable amount of breast tissue due to the transplacental effect of the maternal hormones and there may even be milk production known as “witches milk” in either sex In childhood the breasts are flat, while at the onset of thelarche they become conical. As the breasts become fully developed the inferior part rounds out, while superiorly they become concave. The discrepancy in shape between the superior and inferior aspects of the breast is probably due to varying length and tension of Cooper’s ligaments – hair sized ligaments that provide support from the skin surface to the chest wall. With the aging process, the ligaments stretch or even break, causing the breasts loses support and as a result they sag.
The shape can change significantly with the position of the person, physiological state, and is also dependant on the innate structural makeup of the breast. Thus the firm breast of the adolescent(priotr to pregnancy related change) may change very little with position. The senile breast on the other hand sags due to aging of the normal supporting structure.
The shape of the breast also changes with position so that in the supine position they fall to the chest and sides and flatten, in the decubitus position and prone position they elongate and in the upright position they move downward and flatten.
Although mammoplasty with implants can reproduce and enhance the size of the breasts, reproducing the shape of the breast is a real challenge that is mostly not achieved. Sir Astley Preston Cooper was a British surgeon and anatomist in the late 18th and early 19th century who devoted a large part of his life to the study of the mammary glands. His fascinating and laborious work on the normal anatomy of the breast was published originally in 1840 and is available in electronic version through the Thomas Jefferson U . He observed that breast feeding altered the breast shape so that frequently the breasts became more pendulous in mothers who had breast fed. He also observed that pendulous breasts were more frequent in women from the East and West Indies enabling the mothers to suckle their young who were carried on the mother’s back. By placing the breast over their shoulder or through their armpits the infant had access to mother’s milk while daily chores could be continued. Cooper reported that the same held true for the Hottentots of Southern Africa who nursed their young in similar fashion. Applied Anatomy The breasts are smooth and any evidence of nipple retraction or skin dimpling should raise concern, and careful clinical examination. Even in the absence of a mass by clinical exam appropriate imaging should be performed. Skin dimpling is an ominous sign and most commonly is associated with carcinoma. Peau d’orange is a sign where the skin of the breast is thickened and dimpled like the peel of an orange. It too often reflects an underlying carcinoma. There has been an intense interest in the sculpture called “Night” by da Vinci. The left breast in this sculpture appears to be dimpled or retracted and it has been suggested that the model may have had carcinoma.
|
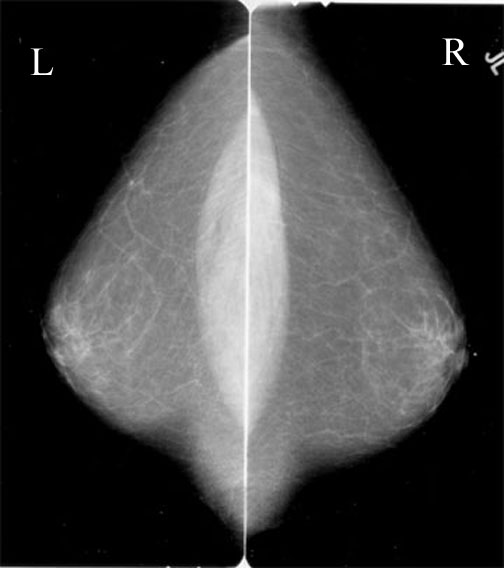 Normal Shape
Normal Shape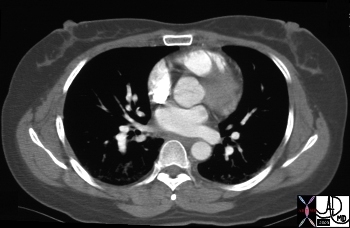
 Young Breast with Support structure Intact
Young Breast with Support structure Intact Aging Breast with Loss Support of Structure
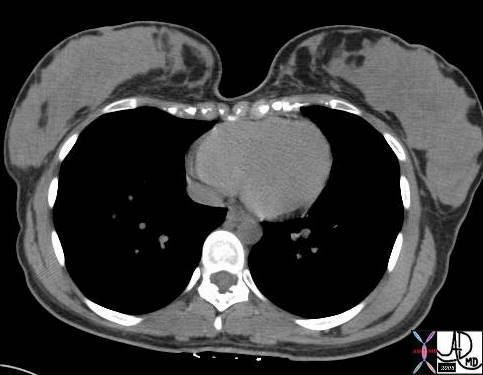
Aging Breast with Loss Support of Structure Position Dependant Shape of the Breasts
Position Dependant Shape of the Breasts Position Dependant Shape of the Breasts
Position Dependant Shape of the Breasts