Introduction
The breast is one of a paired organ system and is an accessory organ of the female reproductive system.
The breast is histologically characterized by alobular structure withcompound saccular glands subtended by a ductal system and supported by intralobular connective tissue that differs significantly from the supporting interlobular connective tissue.
Physiologic changes affect the structural appearance of the tissue
Functionally as an organ of lactation
Overview
Histology of the breast is the description of the tissue structure of the breast including itsconnections relations and growth patterns.
Physiologic changes affect the structural appearance of the tissue.
Principles
In this section we will discuss the principles of the breast as a glandular tissue in general and we will then progress to its specialized structure.
Tissue can be described by its size shape position character. It is made up of characteristic parts which are surrounded by a capsule. For its integrity and functionality it depends on support from other tissues and requires life line type connections to allow it to integrate both structurally and functionally with other tissues. Vascular connections include structures that provide blood supply and drainage. The tissues occupy space and share the space with neighbors The tissues change with time and
specific physiologic events.
The breast is a gland with a lobular organization. Hormonal influence plays a significant role in the cyclical changes of the breast. These changes affect both the structure and function of the breast. Under special circumstances ie pregnancy thelarche remarkable changes in the structure occurs.
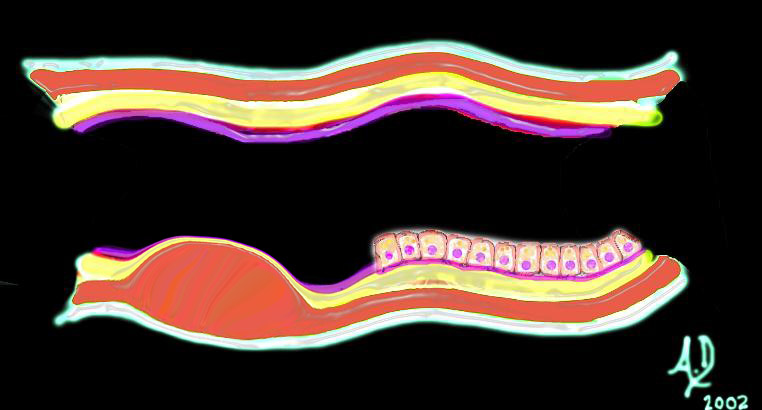
The ductal system obeys the principles of the tube.
Ductal System
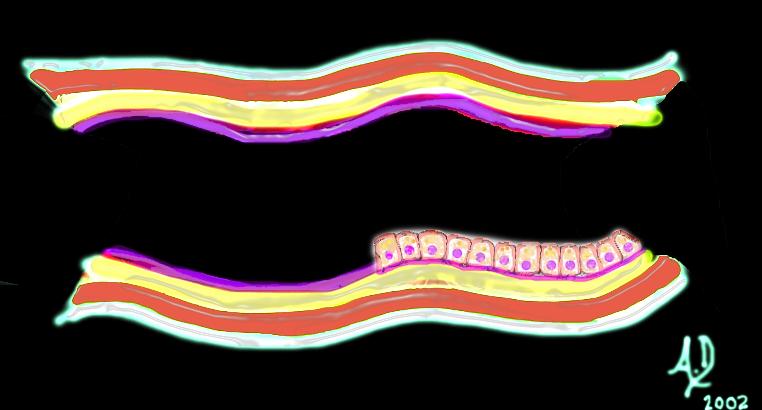
Basic Strcture of Tubular Systems |
| 32347 tube colon small bowel lung bronchus bronchi esophagus stomach large bowel bile duct ureter tube principles Courtesy Ashley DAvidoff MD Davidoff art mucosa submucosa muscularis adventitia serosa histology |
Mucosal Lesion |
| 32347d01 mucosa submucosa muscularis adventitia serosa mucosal mass polyp neoplasm carcinoma acute angles with the lumen histopathology imaging diagnosis Davidoff art Davidoff MD |
|
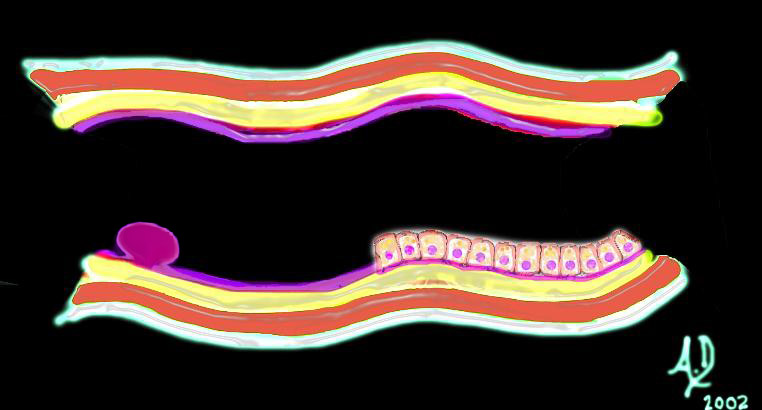
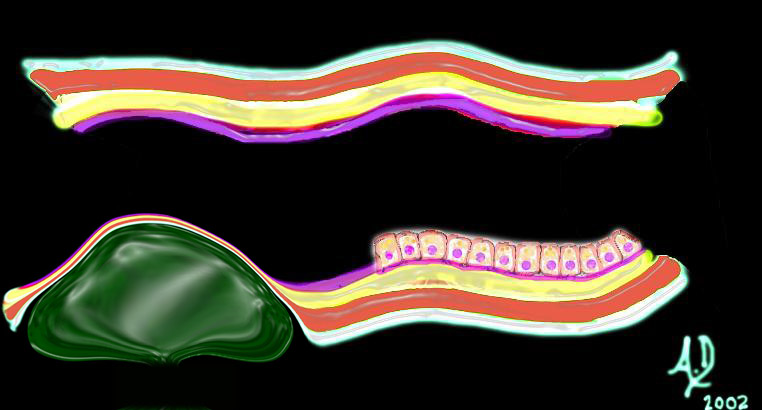
Submucosal Lesion |
| 32347d02 mucosa submucosa muscularis adventitia serosa submucosal mass edema hemorrhage obtuse angles or right angle 90 degree ninety degree angle with the lumen histopathology imaging diagnosis Davidoff art Davidoff MD |
|
Submucosal Lesion |
| 32347d03 mucosa submucosa muscularis adventitia serosa submucosal mass edema hemorrhage obtuse angles or right with the lumen histopathology imaging diagnosis Davidoff art Davidoff MD |
|
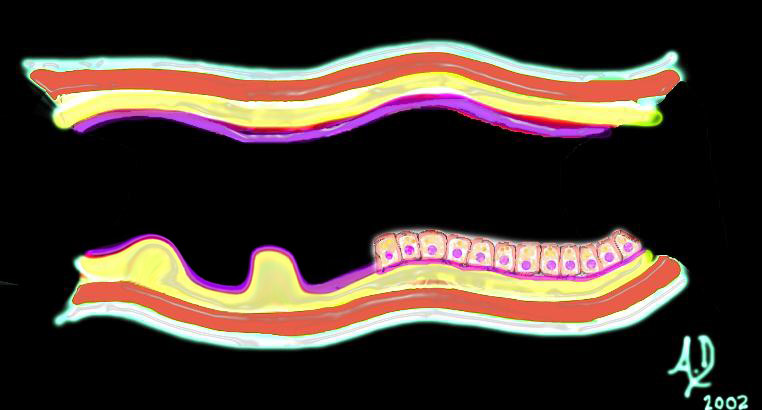
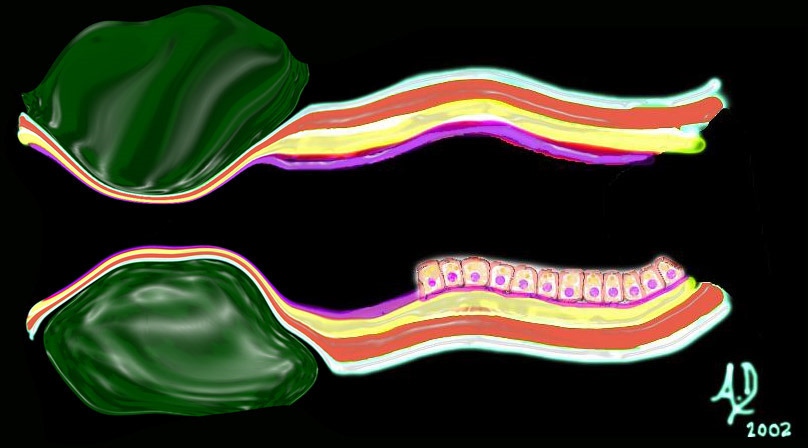
Extrinsic Lesion |
| 32347d04 mucosa submucosa muscularis adventitia serosa submucosal mass edema hemorrhage neoplasm malignancy benign obtuse angles with the lumen histopathology imaging diagnosis Davidoff art Davidoff MD |
|
Circumferential Lesion |
| 32347d06 mucosa submucosa muscularis adventitia serosa submucosal mass edema hemorrhage neoplasm malignancy benign obtuse angles with the lumen circumferential narrowing constriction obstruction histopathology imaging diagnosis Davidoff art Davidoff MD |
Historical Aspects
Early microscopists Malpighi, Marcello (1628-94), Leeuwenhoek, Antoni van (1632-1723), Swammerdam identified microscopic structures but did not recognize cellular composition
1665
Hooke named the cell walled compartments of dead cork tissue
Brown discovered the nucleus.
1838
Schleiden tcell theory’
1839
Schwann tcell theory’
animals were composed of cells concept of structural and functional units
1863
Virchow body as a ‘cell state,’ with specialized categories of cells
1841
Henle first thorough account of human histology.
1830
compound light microscope
1875
Hertwig O. discovery of fertilization of the egg
1876
astigmation was eliminated from microscopic instrumentation improvement in
resolution
Classification
branched apocrine glands
The tissues of the breast derive from ectoderm that invaginate into the underlying mesenchyme
General
The female breast is a dynamic structure that from month to month, more than any other organ, has visble and palpable structural changes. These changes become more dramatic during pregnancy and lactation. The structural changes that are visible and palpable to the patient is often combined with the ever present fear of malignant disease. Many patients therefore have multiple visits to their clinicians and radiologists, to allay or confirm their fears. An improved knowledge of the anatomy and the associated structural changes that occur with the physiology would serve all well.
Size
The lobule is 1 – 8 mm with most lobules being 1 – 2 mm in diameter. Many mature breasts contain adenosis measuring 3 – 9 mm. Lactiferous ducts measure 2 to 4 mm. in diameter while opening pore is about 0.5 mm. Lactiferous sinus measures 5 to 8 mm in diameter.
Shape
There is a radial distribution of the glands and ducts with apex at the nipple and the base toward the chest wall. The gland is a compound saccular gland that becomes almost alveolar when active.
The duct system is lined by sqamous epithelium close to the nipple which abruptly changes to cuboidal epithelium.
Position
There is aradial distribution of the glands and ducts with apex at the nipple and the base toward the chest wall. The lobules are distributed throughout the breast. Acinar lobules are surrounded by intralobular connective tissue which in turn is surrounded by interlobular connective tissue and fat and then skin.
Character
The consistency of the breast tissue as whole is varied depending on the physiologic state and makeup of the breast. It may be soft and loose or firm and rubbery
.
Parts
The glandular substance consists of 15 to 20 lobes each is an independent gland subtended by its own ductal system Each lobe is divided into lobules. The lobe is associated with a duct.
The extralobular terminal duct is lined by columnar cells with a prominent covering of elastic fibers. The intralobular terminal duct is lined by cuboidal cells
In general, lobules include acini and terminal ductules, whereas ducts comprise of interlobular ducts and ducts further downstream. The epithelial structure varies in appearance depending on physiologic state but has an inner layer of secretory cells and an outer layer of
myoepithelial cells. During pregnancy there is budding-off at the ends of existing duct within the
lobule to become a simple cuboidal epithelium the acini expand at the expense of the intralobular stroma.
The ducts branch dichotomously forming terminal ductal lobular
Skin and Connective tissue capsules
The capsule at large is the skin areola and the nipple the lobule also has a capsule areolar and nipple has thin pigmented epidermis. In the dermal layer there are smooth-muscle fibers in circular and radial orientation. The nipple has mostly circular muscle which extends to ducts. The areola contains
Montgomery glands which are branched apocrine glands. The lobule is surrounded by a dense
collagenous fibrous structure.
Support
The lobules are supported and surrounded by interlobar connective tissue and in turn is surrounded by interlobar dense connective tissue with elastic fibers structure and variable amounts of fat and finally
fat and then skin. The intralobular supporting connective tissue has a myxomatous nature loose and fine in texture cellular and vascular and contains no fat. The interlobular connective tissue is relatively
abundant, dense and coarse. During pregnancy interlobular fat disappears to make room for lobular expansion.
Blood Supply
The arterioles form a plexus in the submucosa and extend into the mucosa and the
Muscularis. The capillaries deliver the blood to the layers of the wall. It is unlikely that the
blood vessels penetrate the muscularis mucosa. The cells of the epithelium are therefore supplied via the interstium rather than by direct supply by arterioles
Nerve Supply
The breast is supplied by the 2nd through 6th intercostal nerves which provide sensory and
sympathetic fibers. There is a rich nerve plexus supplying the smooth muscles of the ducts and
and a supply to the myoepitelial cells in the acini.
Venous Drainage
Venous drainage of the breast is usually is via ………..text
Variations include ……………Text
Lymphatic Drainage
The breast has a very rich supply of lymphatics with the axilla containing the large majority of the lymphatic drainage from the breast. There is a superficial set of lymphatics aka subareolar plexus in the skin and a deep or fascial set. Both follow the fascial connective tissue around the lobules and around the ducts. The rich lymphatic network is in the submucosal layers of the epithelium and the lympatics course along the connnective tissue framework
Ducts
The acini are subtended by the ductules. The acini form a conglomerate group called the lobule which are subtended by the intralobular ductules and interlobular ducts.which drain into the extralobular duct. Multiple extralobular ducts join to form 8-20 ducts that wid to form a sac (ampulla) or lactiferous sinus just prior to the opening onto the nipple. In general, lobules include acini and terminal ductules, whereas ducts comprise of interlobular ducts and ducts further downstream. Due to the substantial individual variations under the influence of hormones, distinction between lobules and ducts is surprisingly sometimes arbitrary at the microscopic level.
Downstream ducts include in order;
main extralobular duct
lactiferous duct
lactiferous sinus
narrows to open at the summit of the nipple
The mouths of main lactiferous ducts have a stratified squamous epithelium The major breast ducts are
lined by pseudostratified columnar and then double layered cuboidal epithelium epithelium supported by
myoepithelial cells. In the menstrual cycle during the height of estrogen and progesterone activity the epithelium and stroma both proliferate. By the end of pregnancy there is a dominant proliferation of glandular elements lined by cuboidal cells. There is a regression of these glands following termination of lactation.
Relations
The breast lies anterior to the pectoralis major and serratus anterior muscles. More anterior to the muscles is the prepectoral fascia, then the retromammary fat and then the glandular tissue. The glandular tissue is surrounded by fibrous tissue and fat.
Connections
Embryology
Breasts begin developing in the embryo about 7 to 8 weeks after conception. At this stage they consist of a ridge of tissue. From weeks 12 to 16, small groupings of cells begin to branch out laying the infrastructure for future ducts and glandular tissue. Smooth muscle cells group to help form the nipple and the areola. Maternal hormones cross the placenta in the later stages of pregnancy, stimulating cells to organize into primitive ductal system. In the final 8 weeks, lobules, mature and begin to secrete colostrum. The secretions cease in the first few weeks of life. These changes occur in both male and female fetuses resulting in prominent breast tissue that can be palpated beneath the nipples.
Growth and Aging
With the onset of puberty and over the next four years, the release of estrogen and progesterone, and also under the influence of the hypothalamus, anterior pituitary, and ovaries: also requires insulin and thyroid hormone initiate further development, usually completed by age 16. Further maturation of the breast tissues occurs with lactation