Character
The adipose tissue in general makes up 80-85 % of the breast gives it a soft feel and together with the stroma and glands the breast is characterized as having a rubbery feel. However, in general, the glandular portion of the breast has a firm, slightly nodular feel, while the fat is almost always soft.
As we have noted above there are breasts where 80% of the breast is fibroglandular and others where the fat predominates. It is more common to see the dominance of fat in the breast of older patients, and fibroglandular dominance is usually seen in the young, though there is wide variation.
The breasts become firmer in pregnancy and lactation, but become softer and less rubbery with aging, mostly due to glandular regression and proliferation of fat.
Consistency of breast lobes varies from woman to woman, and will vary during the cycle, and may even vary in an individual from one side to the other.
The ducts of the breast are usually not palpable unless they are engorged with milk, inflamed or contain a tumor.
The areola is of a delicate rose colored hue in the nulliparous patient but enlarges and darkens with pregnancy, and may even become black. After pregnancy it may lighten but it never returns to its former rose colored hue. The nipple also starts out as rose-colored structure, usually being slightly darker than the areola and darker than the skin. It also darkens with pregnancy.
Applied Anatomy
The discrepancy in textures between the adipose tissue and the mammary apparatus, allows one to outline the lobes by carefully palpating the breast. When the breasts feel thick and lumpy the entity of fibrocystic change probably exists. This finding implies that the fibroglandular elements are enlarged. This enlargement is not necessarily abnormal.
The finding of a mass or a focally enlarged and hardened part of the breast is a significant finding and further characterization is important. It is essential to determine the mobility of the mass and get a feel as to whether it is tender (usually a finding in benign disease) whether it is fixed to the skin or deep muscles (a bad sign) and whether there are associated findings such as other masses, nipple discharge, or regional axillary adenopathy.
The radiographic difference in density between the parenchymal tissue and the fat allows structural evaluation and forms the basis for mammographic imaging, US imaging CT scanning and MRI.
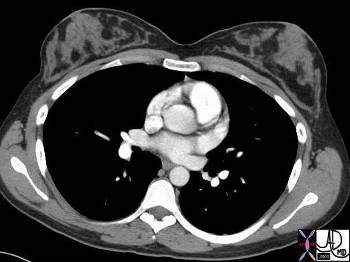
Combination of Adipose and Glandular Components |
| This normal CT scan of a 24year old female shows the difference between the soft tissue density of the glandular and stromal tissue on the one hand (gray structures of the breast) and the adipose tissue of the breast on the other (charcoal black) Courtesy Ashley Davidoff MD 42675 |
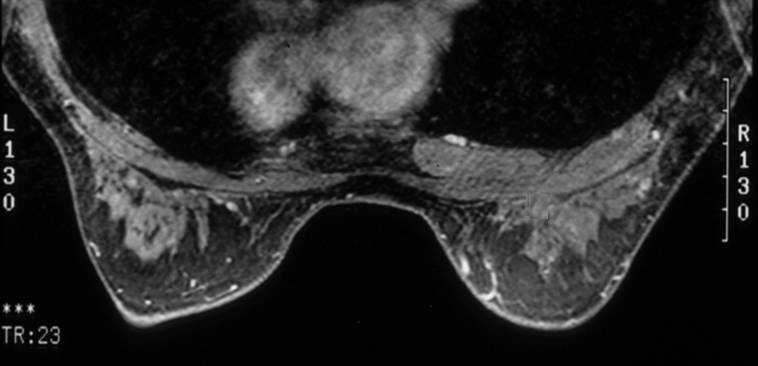 Combination of Adipose and Glandular Components Combination of Adipose and Glandular Components |
| The intrinsic differences in the proton density of the mammary apparatus and adipose tissue enable distinction on the MRI scan. In the image above the fat of the breast is relatively dark due to fat suppression techniques, and the mammary apparatus is gray. Within the mammary apparatus the distinction between stromal tissue and glandular tissue cannot be made. Courtesy Priscilla Slanetz MPH 42825b01 |
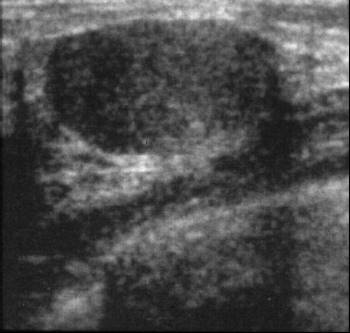
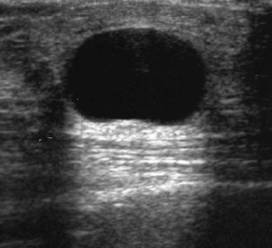 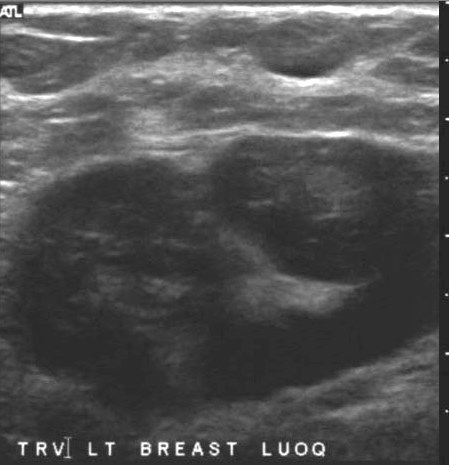 Cystic and Solid Lesions Cystic and Solid Lesions |
| The strength of ultrasound technology in the breast is its ability to define the nature of palpable masses. In the first example above a palpable mass is clearly characterized as a cyst with its anechoic nature and through transmission, whereas the lesion on the right is clearly a complex and solid lesion. Ultrasound in the breast is used to answer specific focused questions – cystic or solid? Courtesy Priscilla Slanetz MD MPH 42883 4284 |
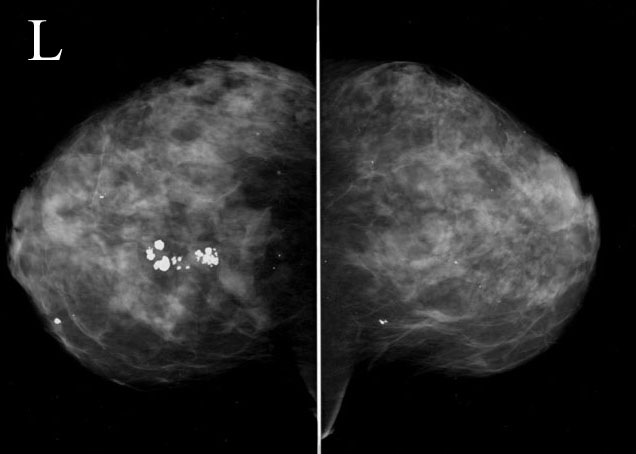
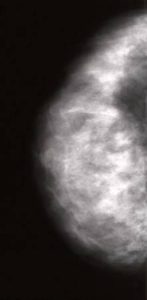 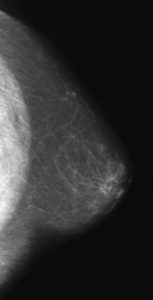 Dense Breast and Fatty Breast |
| Mammography is a high resolution technique that is best suited for identifying subtle masses, calcifications, and architectural distortions. Image 1 reveals a dense breast meaning that the fibroglandular elements dominate and the breast in image 2 represents a fatty breast. 42868 42864 Courtesy Priscilla Slanetz MD MPH |
Diseases
Carcinoma
Masses
An irregularly shaped mass, particularly if spiculated, is concerning for malignancy. A spiculated lesion is concerning whether it is identified on mammography, ultrasound, MRI or CT. The density of malignant lesions is also slightly greater than soft tissues. The high density of a carcinoma is characteristic of the scirrhous carcinoma.

Mass in the Right Breast |
| This mammogram is blatantly positive for a dense, irregularly shaped mass that extends to, and involves the chest wall. Most cases are far more subtle than this case. The patient had an inflammatory breast carcinoma. Note that by convention mammographic images are projected with the left breast to your left and the right breast to your right – the opposite to the projections of cross sectional images. Courtesy Priscilla SlanetzMD MPH 42747 |
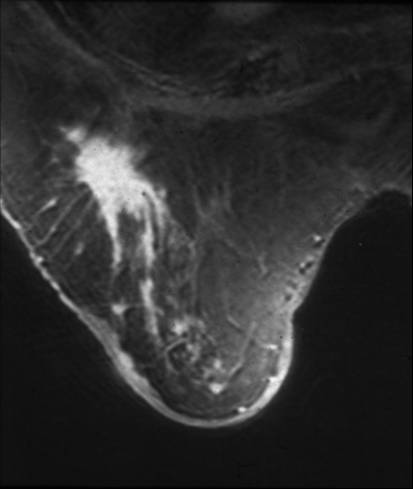 Spiculated Mass in the Right Breast Spiculated Mass in the Right Breast |
| This is an MRI of the right breast of a 78 year old patient with a remote history of invasive lobular carcinoma. The finding on the MRI is characterized by an enhancing spiculated mass. Recurrent carcinoma was present at pathology. Courtesy Priscilla Slanetz MD MPH 42977 |
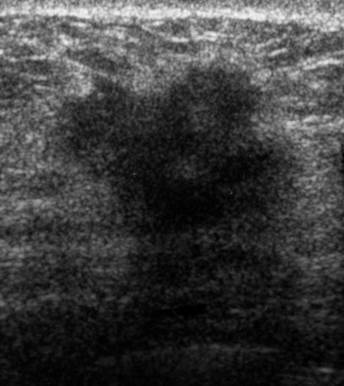
Hypoechoic Mass with Irregular Borders |
| This US reflects a hypoechoic solid mass that is characterized by an irregular border. A feature that is highly suggestive of malignancy. The pathology on this case was an invasive ductal carcinoma. Courtesy Priscilla Slanetz MD MPH 43004 |
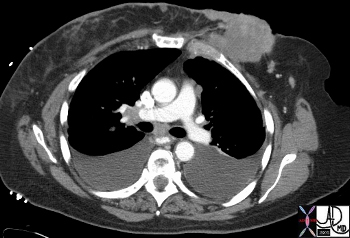
Aggressive Mass Invading the Chest Wall |
| The CT reveals an obviously aggressive lesion in the left breast of a 66year old female. It is extending as an irregular mass invading the chest wall posteriorly and projecting through the skin anteriorly. Courtesy Ashley Davidoff MD 43615 |
Calcifications
Calcifications that are associated with malignancy are usually small (<0.5 mm). A magnifying glass is an essential tool to evaluate the breast since the malignant calcifications may be too small to see with the naked eye. The calcifications are characterized by their pleomorphic shape, meaning that they have a heterogeneous nature. They may be fine and granular, and or linear, and or branching. Their distribution is also varied so that they could be clustered, regional, diffuse, or segmental.
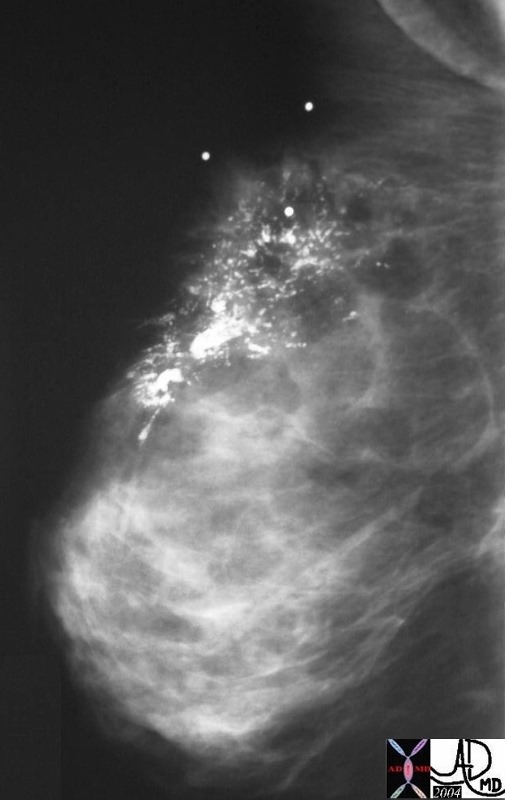 Pleomorphic Calcifications – Carcinoma Pleomorphic Calcifications – Carcinoma |
| This mammogram was positive for carcinoma. The structural feature that suggests malignancy is the heterogeneity of the shapes and sizes of the calcifications. This type of calcification is termed “pleomorphic” calcification. The final diagnosis was intraductal carcinoma. Courtesy Priscilla Slanetz MD MPH 27 |
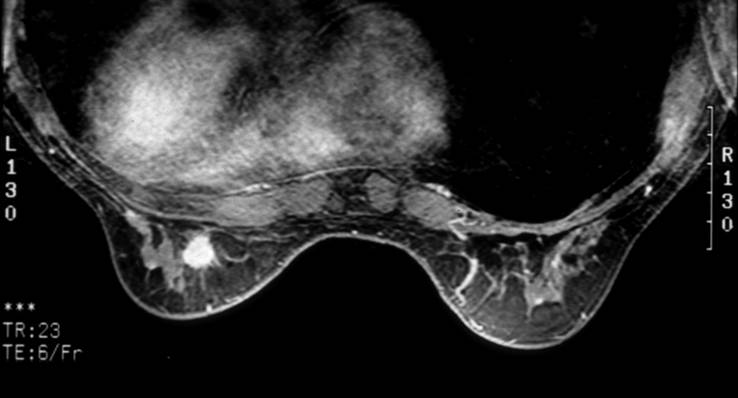 Hypervascular with Stellate Morphology- Carcinoma Hypervascular with Stellate Morphology- Carcinoma |
| The finding on this contrast enhanced MRI is a mass in the left breast that is hypervascular and has a spiculated border. The pathology in this case was an invasive intraductal carcinoma. Courtesy Priscilla Slanetz MD MPH 42982 |
Benign diseases
Benign breast masses are common and include predominantly fibroadenomas and fibrocystic disease. Cysts are part of the fibrocystic group of diseases.
Fibroadenomas are the most common breast lesion particularly in women under the age of 40. It is a benign neoplasm of the stromal and epithelial elements. The characteristic finding of a fibroadenoma is its smooth borders on mammography and US.
| Fig. 1 Fig. 2
Smooth Margins- Benign Features |
| A mammogram on the left shows an ovoid mass which is hypoechoic with smooth margins. These findings are characteristic of a benign lesion and could represent a cyst or fibroadenoma as the most likely causes. The US on the right shows a well circumscribed solid mass characteristic of an adenoma. Courtesy Priscilla Slanetz MD MPH 42913 42914 |
 Popcorn Calcification- Benign Features Popcorn Calcification- Benign Features |
| This mammogram shows large popcorn shaped calcifications in the left breast characteristic of an involuting fibroadenoma. 42748 Courtesy Priscilla Slanetz MD MPH |
Relations
The mammary apparatus itself is completely surrounded by adipose tissue with a superficial layer lying deep to the dermis and the retromammary layer lying anterior to the pectoralis major muscle. Outside of the breast proper, the most important structural relation of the breast is the pectoralis major muscle and its fascia which form the posterior border of the breast. The serratus anterior to lesser extent also forms a part of the posterior border. Its other borders include the clavicle superiorly, the sternum medially, 6th and 7th rib inferiorly.
Applied Anatomy
The involvement of the pectoralis fascia by a malignant mass is an important consideration in the staging of breast carcinoma which was discussed above. The pectoralis muscle can be identified by CTscan, MRI and also by ultrasound.
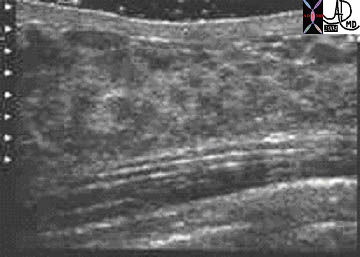
Chest Wall Anatomy |
| This ultrasound image shows the deep structures of the breast – most posteriorly is the pectoralis muscle, the prepectoral fascia, (thin white lines) retromammary fat which is relatively hypoechoic, the nodular appearance of the glandular tissue and the skin. Courtesy Ashley Davidoff MD 43848 |