| Ducts and ductules
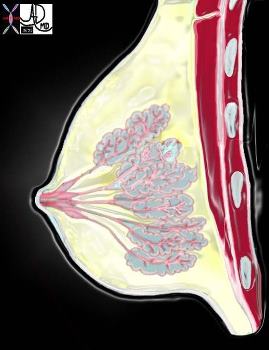
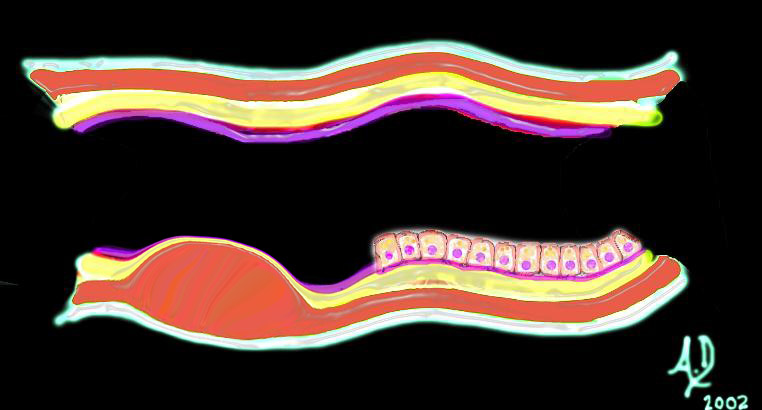
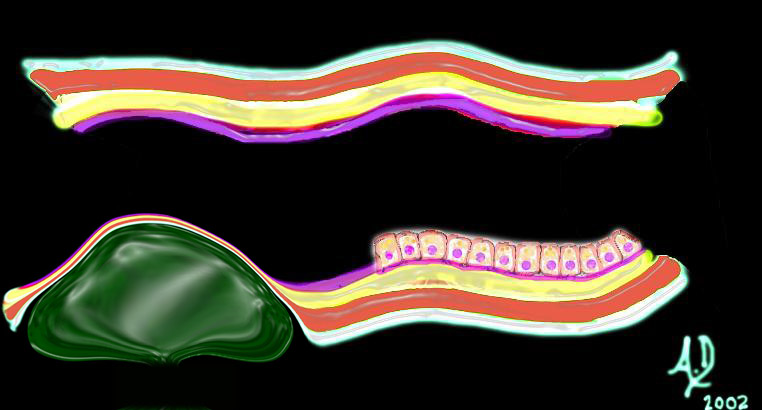
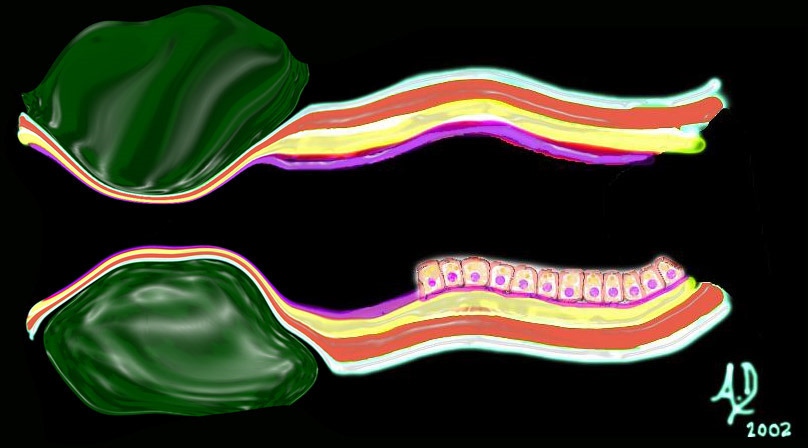
The duct of one gland or lobe is called the lactiferous duct. This duct has a small region of focal dilatation (measuring 2-4mms) called the ampulla (aka lactiferous sinus) present just before it enters the nipple. The ampulla serves as a reservoir for the milk. Each of the 15-20 ducts perforates the nipple with a separate relatively narrowed orifice. The lactiferous duct branches into segmental ducts which in turn give rise to the subsegmental ducts. The terminal portion of the subsegmental duct is called the extralobular terminal duct and it gives rise to the intralobular terminal duct as it enters the lobule. Each intralobular terminal duct enters an acinus of which there are many in a lobule.
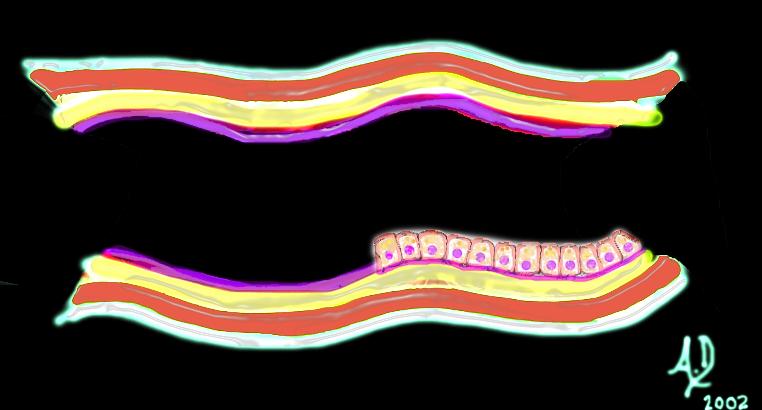
At a histological level, the lactiferous duct is composed of two layers of cells – a basal cuboidal epithelium and a luminal columnar epithelium. In addition there is are both longitudinal and transverse elastic fibers. Branches of the lactiferous duct are lined with a simple cuboidal epithelium. Due to the substantial individual variations under the influence of hormones, distinction between lobules and ducts is, surprisingly, sometimes subjective at the microscopic level. The acinar structures achieve full physiologic development only with pregnancy. During lactation, the alveolar cells secrete milk which is carried to the nipple via the ducts, and is expressed with the aid of the smooth muscle components which are stimulated by the sucking reflex.
Diseases Principles
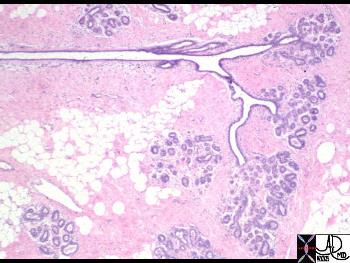
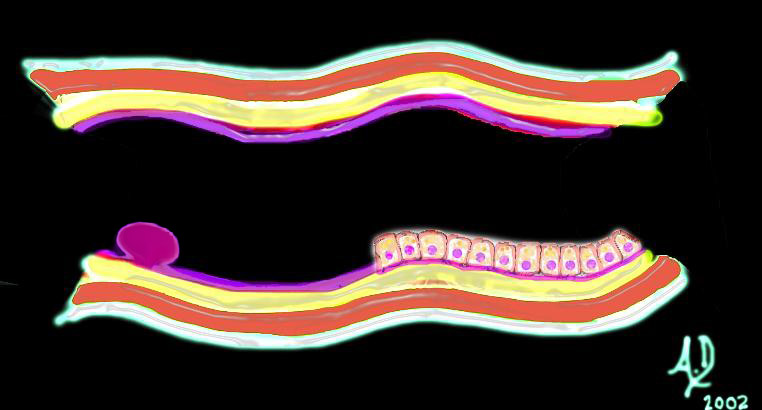
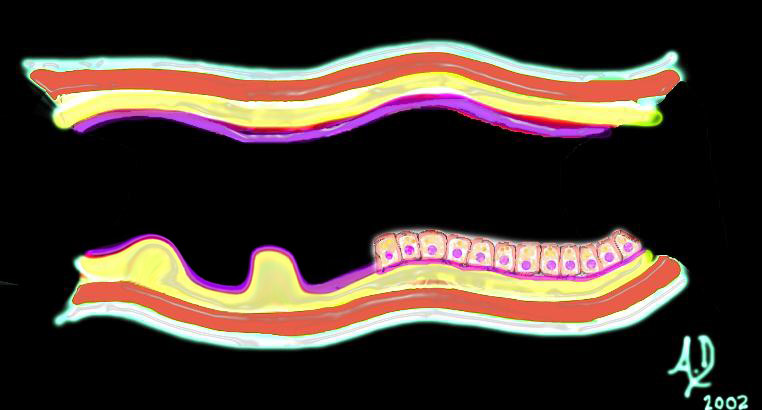
Malignant breast disease Most diseases both benign and malignant arise from this highly active terminal ductal lobular unit (TDLU) in which there is constant change of structure. (Stirling) The carcinomas are the most significant lesions of the breast. There are two major types of breast carcinoma that arise from the lobule namely ductal carcinoma and lobular carcinoma. They both arise from the TDLU. Carcinoma of the breast at this level is divided into the non invasive or “in situ” carcinomas on the one hand and the invasive carcinomas on the other. The “in situ” carcinomas are restricted to the lobule and do not show invasion of the basement membrane while in the invasive group, there is obvious transgression of the basement membrane. The “in situ” group has variable behavioral patterns and outcomes. These lesions may remain dormant for a lifetime, or may even involute. They do however place the woman at increased risk of developing cancer and should therefore be treated with heightened awareness. The two types of “in situ” carcinomas are called ductal carcinoma in situ (DCIS), and lobular carcinoma in situ. (LCIS) and they are very different. DCIS is common and occurs in 70-95% of women at autopsy and is commonly associated with microcalcifications on mammography. It arises from ductal epithelium. LCIS is less common, clinically and radiologically more elusive, occurs in 1-5% of biopsies, and is rarely associated with microcalcifications on mammography. Wellings Once LCIS is identified the risk of developing cancer if untreated is about 30% within 20 years of diagnosis. It is not considered a precancerous disease, but a marker of increased risk. The invasive carcinomas of the breast are correspondingly called invasive ductal carcinoma and invasive lobular carcinoma and are defined by the transgression of the basement membrane by malignant cells. The most common site of involvement is the upper outer quadrant since as we have learned it is the location of “extra” tissue called the axillary tail of Spence. The presence of a larger amount of glandular tissue raises the relative incidence of disease in this quadrant. About 45% of carcinomas arise from this upper outer quadrant. Invasive ductal carcinoma is the most common type of carcinoma and it has a tendency to incite a fibrous response which has structural consequences. Firstly fibrous tissue is very dense so that this type of tumor has a relatively dense appearance on mammography. The scirrhous and desmoplastic nature of fibrosis also causes a tugging effect on other structures such as the Cooper’s ligament, the skin or the nipple so that retraction of these structures can occur. Peau d’orange is the dimpling of the skin in carcinoma that is reminiscent of the dimpling seen in the skin of an orange, and it is caused by the effect of the carcinoma on the ligaments of Cooper. New onset of nipple retraction is also an important warning sign of cancer.
Fibrocystic disease Fibrocystic changes in the breast are the most common entity of the breast and accounts for the common lumpy bumpy feel of normal breast tissue. It is a benign entity that arises from the TDLU. The pathology is caused by proliferation of the connective tissue and or epithelial tissue, resulting in cystic change and or fibrous changes. It has a variety of clinical, imaging and pathological variations including a single dominant cyst, diffuse irregularity caused by fibrocystic change and diffuse irregularity with a dominant lesion (U Virginia) The entity is subject to morphologic changes with hormonal changes of the menstrual cycle, and it may be associated with pain. The lesion is most common in the upper outer quadrant where the lobules are more voluminous in the tail of Spence.
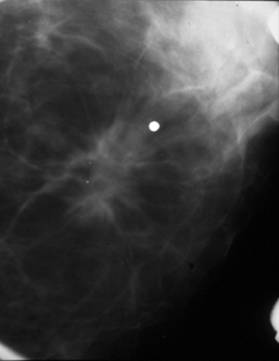
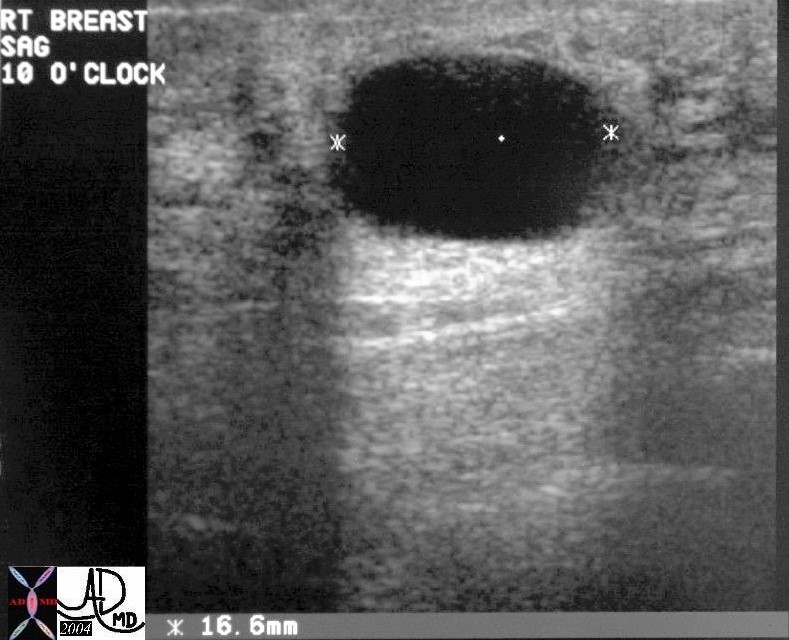
A cyst is noted on this ultrasound in the breast of a young woman with a palpable mass. This entity is part of the fibrocystic entity discussed above and most commonly presents as a disturbing mass. Ultrasound is the study of choice when this condition is clinically suspected. Note that the cyst has no internal echoes, the wall has no evidence of neither focal nor diffuse thickening and there is superb through transmission of sound. Courtesy Priscilla Slanetz MD MPH 28241 Fibroadenoma Fibroadenoma is a common benign disorder of younger adult women that arises from the intralobar connective tissue elements and from epithelial elements. Unlike the cyst above the fibroadenoma presents on ultrasound as a well circumscribed solid lesion.
Diseases of the ducts
Nipple discharge Nipple discharge is the third most common breast symptom after mass, and pain of the breast. Discharge is a normal event in women who are in the reproductive age. 50-60% of women can express some secretion on self examination. It is uncommon that a discharge is associated with breast cancer. Causes of nipple discharge include persistent secretion after pregnancy, benign hormonal affects, and mammary duct ectasia. Phenothiazines may also cause a nipple discharge. Benign features include bilaterality, and the involvement of multiple orifices. Bloody discharge that is spontaneous, from a single duct should raise concern for malignancy, but even so, only 10% of these patients have an underlying malignancy. Intraductal papilloma is the most common cause.
Paget’s disease of the nipple Paget’s disease of the nipple is a rare disease of the nipple characterized by eczematous change of the nipple and almost always associated with an underlying breast carcinoma, specifically with high grade DCIS. The areola may also show eczematous change. It occurs in about 12% of patients with breast carcinoma. The findings in the nipple may be the only indication of disease, and so a new scaliness of the nipple warrants serious attention of clinician, mammography technologist, and radiologist. Only about 50% of patients with Paget’s have a radiographic abnormality on mammography. |