Author Lisa Wiechmann MD
Overview
Breast cysts are epithelial-lined cavities containing fluid and represent an involutional disorder; they are considered a non proliferative lesion of the breast by the current classification by Page ( Benign breast disorders and disease- see table). Breast cysts occur frequently, are often multiple and usually present in younger women. They usually present as palpable, mobile, firm masses which contain non-bloody fluid when aspirated and are well demarcated from the surrounding tissue. Their pathogenesis is related to abnormal involution of the lobular epithelium. Cysts tend to fluctuate with the menstrual cycle.
Classification
Breast cysts are part of the non-proliferative disorders of the breast which in turn account for approximately 70% of benign breast conditions. Other non-proliferative disorders include duct ectasia, periductal mastitis, fibroadenomas and related disorders. The classification of breast cysts is based on histology and size (Macrocysts and microcysts). Typically they are constituted by simple flattened cuboidal epithelium with apocrine metaplasia.
Statistics
Breast cysts represent the most common cause of a palpable lesion of the breast in women age 35-55 and are thought to be present in approximately 7% of the population (Haagensen) .Cystic change in the breast is a very common finding during autopsy (Davies : 58% microcysts, 21% cysts > 1cm)
Sex Distribution
female disease
Age Distribution
Breast cysts are common in younger women. Because of the hormonal fluctuations around menopause, women often present during the perimenopausal years. Cysts, however, can occur at any age, even in postmenopausal women. Usually these postmenopausal women are taking hormone replacement therapy (HRT).
Pathogenesis
The pathogenesis of breast cysts is related to abnormal involution of the lobular epithelium. Involution of lobular epithelium depends on the surrounding stroma and at times the two processes (involution of stroma and parenchyma) are not integrated. If the stroma involutes too quickly, acini within a lobule distend and become microcysts which may in turn become macrocysts.
Result
A breast cyst is a space occupying mass which is palpable on breast examination
Complications
Simple cysts carry no malignant potential, but complex cysts, recurrent cysts, cysts that do not undergo complete resolution after aspiration, or cysts that upon aspiration contain blood may need to be biopsied to exclude intracystic carcinoma. If the cyst fluid showed atypical cells on cytology, repeat examination 4-6 weeks after aspiration is necessary to exclude recurrence of the cyst. A recurrent cyst with atypical cytology is typically surgically excised.
Natural History
The breast goes through different physiologic stages: adolescence, pregnancy, lactation and senescence. The pathogenesis of breast cysts is related to abnormal involution of the lobular epithelium. Involution of lobular epithelium depends on the surrounding stroma and at times the two processes (involution of stroma and parenchyma) are not integrated. If the stroma involutes too quickly, acini within a lobule distend and become microcysts which may in turn become macrocysts.
Gross Pathology
Cysts are epithelial lined cavities containing fluid. They are common in women aged 35-55 years and their presence is thought to be secondary to abnormal breast involution. They can be single or multiple, unilateral or bilateral and they often fluctuate in size with the menstrual cycle. Macrocysts are large enough to produce palpable masses (Haagensen). Cysts are often blue (blue dome cysts) in the fresh state and are surrounded by fibrotic stroma.
Histopathology
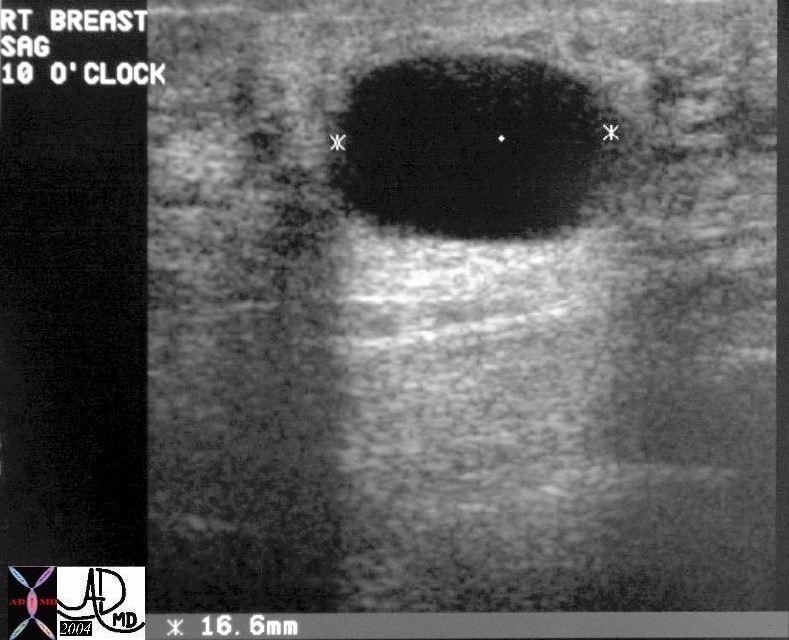
Cysts are epithelium lined cavities. The epithelium is composed of two layers : an inner ( luminal) layer and an outer ( myoepithelial) layer. It can be metaplastic (apocrine metaplasia) or extremely attenuated.
This high power view is of a histological section from the records of a patient with a serous cystadenoma of the pancreas. The lumen of the cyst is at the top of the image and is cream colored with floating debris. A single layer of columnar epithelial cells lines the cyst. A pseudocyst on the other hand would have no epithelial lining.15317 Courtesy Barbara Banner MD The CommonVein.net
Cytopathology
The lining epithelium at times shows apocrine metaplasia which is characterized by eosinophilic granular cytoplasm and has protrusions into the luminal border called”apocrine snouts”.
Clinical Presentation
Microcysts can be asymptomatic or present as nonspecific breast tenderness whereas macrocysts ( >1cm) are usually palpable.
Imaging
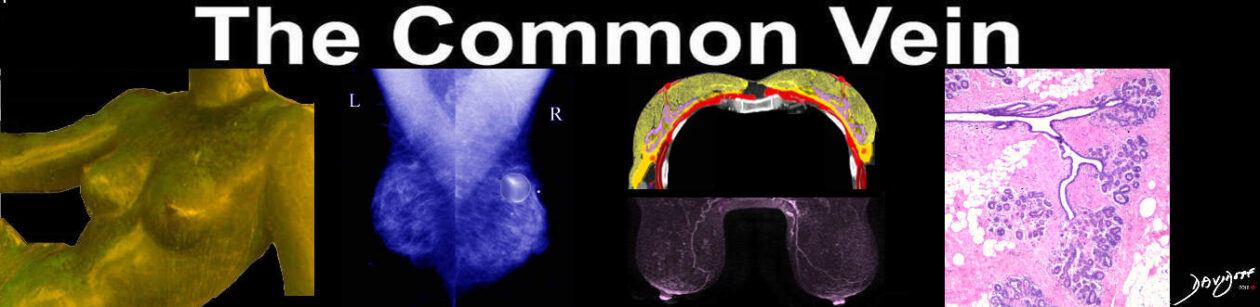
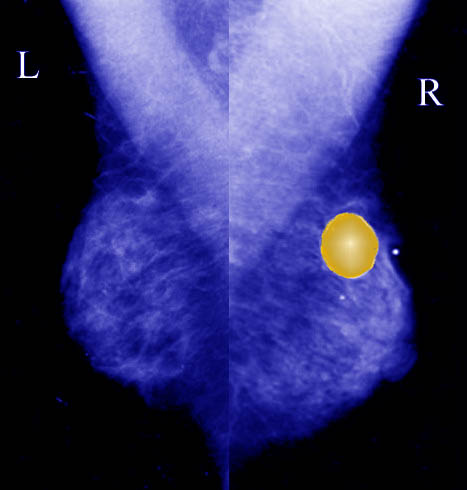
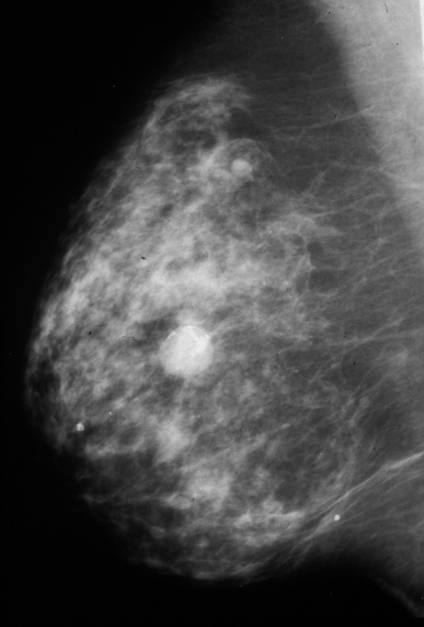
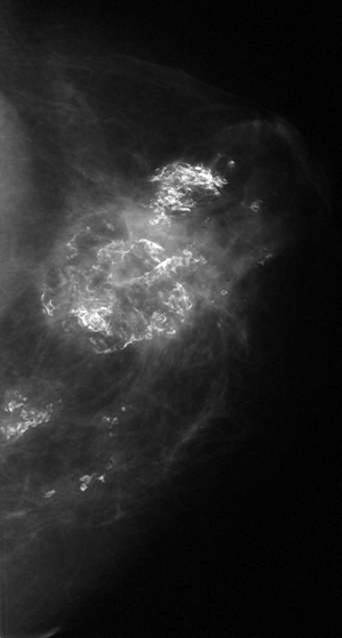
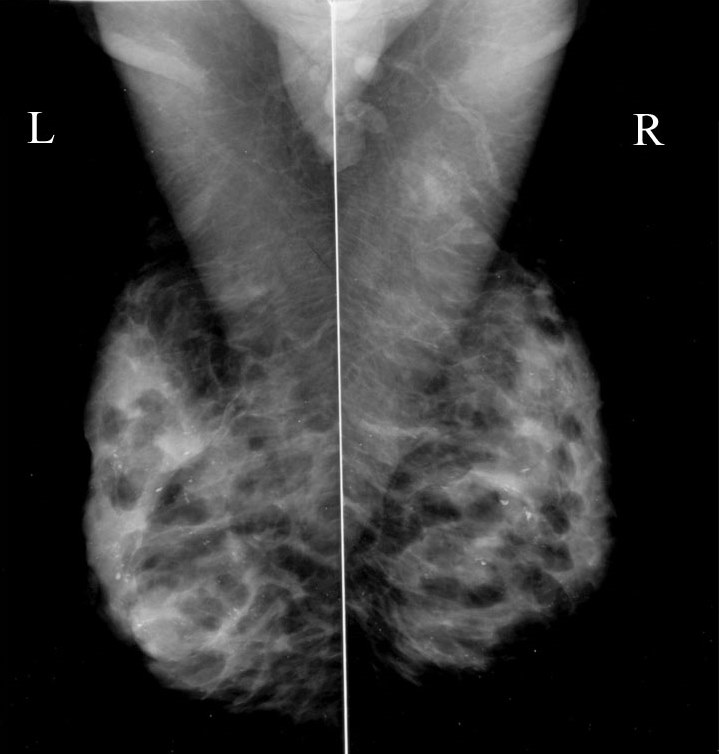
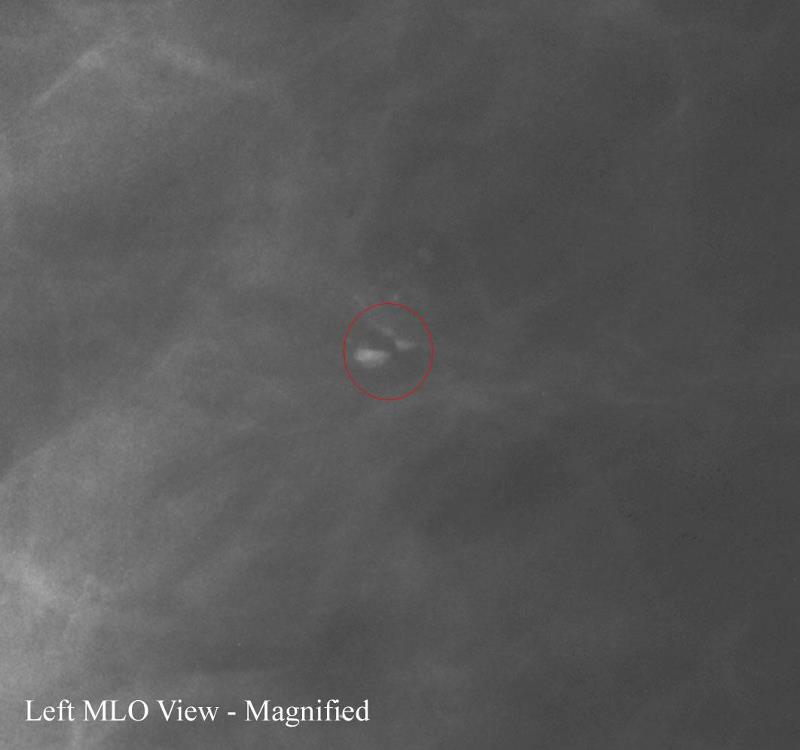
Mammographically cysts appear as well-circumscribed low attenuation or isodense masses that may have rim calcifications or layering calcifications suggestive of “milk of calcium”.
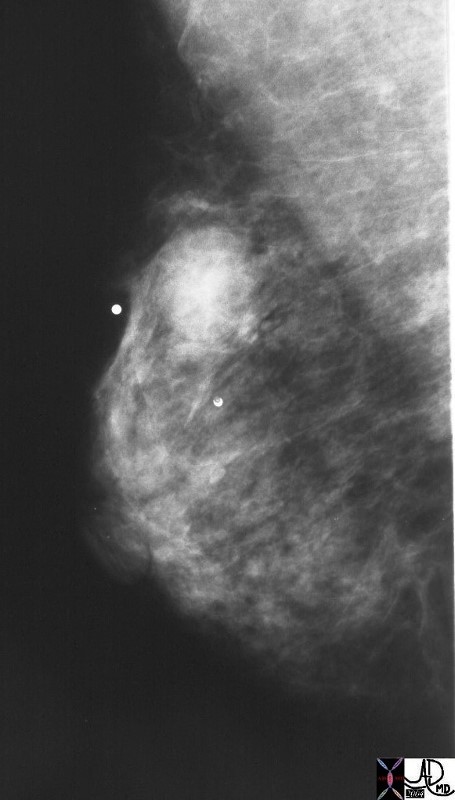
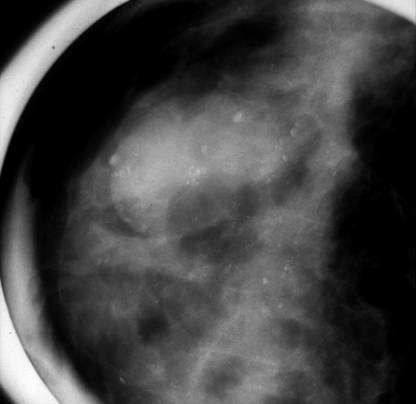
Cystic lesions that may have any complexity need to be aspirated and evaluated.
Milk of calcium represents calcium which has precipitated out from the concentrated cyst fluid and is floating within the fluid. When the patient is imaged in different positions, the calcium will layer in the most dependent portion of the cyst.
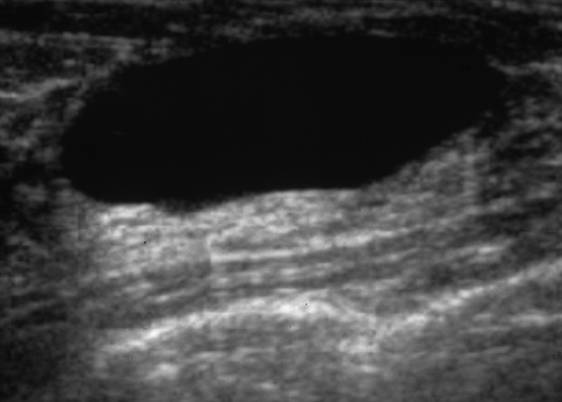
Not all cysts need to be aspirated. Aspiration is only performed on a simple cyst if the patient is extremely symptomatic. Cystic lesions that are not completely anechoic are often aspirated to exclude a solid mass. Fluid is only sent to cytology if the patient requests it, the fluid appears to be bloody, or the cyst does not completely resolve with aspiration. If atypia is seen in the cyst fluid, this most commonly is due to peri-cystic inflammation, a benign process in the breast. However, in rare cases, the atypia is a sign of a more serious problem such as malignancy. When atypia is seen on cytology, follow-up imaging in 2-3 months of the area that underwent aspiration is performed. A recurrent cyst on the follow up images warrants surgical excision.